ateneo hospitalario - ministerio de salud · paciente sexo femenino de 44 años, ingresa en julio...
TRANSCRIPT
SERVICIO DE HEMATOLOGÍA
HIGA GRAL. SAN MARTÍN
LA PLATA
MAYO DE 2013
ATENEO HOSPITALARIO

CASO CLÍNICO
� Paciente sexo femenino de 44 años, ingresa en julio de 1998 por presentar astenia, disnea clase funcional III, fiebre y tos seca de 7 días de evolución
� Antecedentes personales:� HTA en tratamiento con enalapril
� Tabaquista: 10 cigarrillos/día desde los 16 años

CASO CLÍNICO
� Examen físico:
� Piel y mucosas ictéricas
� Fauces eritematosas
� Ap. Respiratorio y Cardiovascular s/p
� No se palpan adenopatías ni visceromegalias
� Laboratorio de guardia:� Hto: 19%, G.B 7.500/mm3, Plaq: 250.000/mm3, TGO 25 U/l,
TGP 18 U/l, suero ictérico
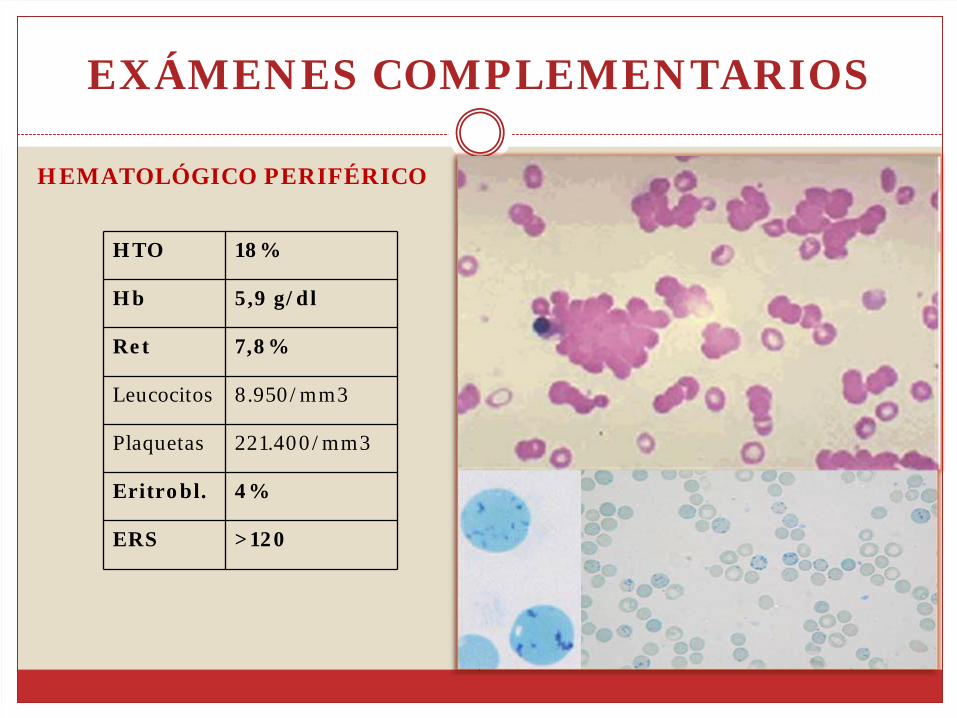
EXÁMENES COMPLEMENTARIOS
HTO 18%
Hb 5,9 g/dl
Ret 7,8%
Leucocitos 8.950/mm3
Plaquetas 221.400/mm3
Eritrobl. 4%
ERS >120
HEMATOLÓGICO PERIFÉRICO

EXÁMENES COMPLEMENTARIOS
Panaglutinina de tipo IgM, activo a 4°C y 20°C, de
especificidad anti I
Títulos 4°C: 16.38420°C : 1.024
Estudio Inmunohematológico
DIAGNÓSTICO
ANEMIA HEMOLITICA AUTOINMUNE POR ANTICUERPOS FRIOS
IDIOPATICA
SECUNDARIASíndromes Linfoproliferativos CrónicosNeoplasiasInfeccionesM. pneumoniaeMononucleosis infecciosaOtras

EXÁMENES COMPLEMENTARIOS
� Rx de tórax: infiltrado intersticio alveolar bilateral
� Eco abdominal: normal
� Serologías: HIV, VHB, VHC negativas.
E. Barr, VHS, CMV, Toxo: IgG positivas

ANEMIA HEMOLÍTICA AUTOINMUNE POR ANTICUERPOS FRÍOS SECUNDARIO A INFECCIÓN

TRATAMIENTO
� Ambiente cálido
� Transfusión 2 USG
� Acido fólico
� Tratamiento antibiótico con Ceftriaxona + Claritromicina
� Buena evolución clínica, disminución de los títulos de crioaglutininas
Hto 30% PCD + Franca mejoría de los parámetros de hemólisis
ALTA
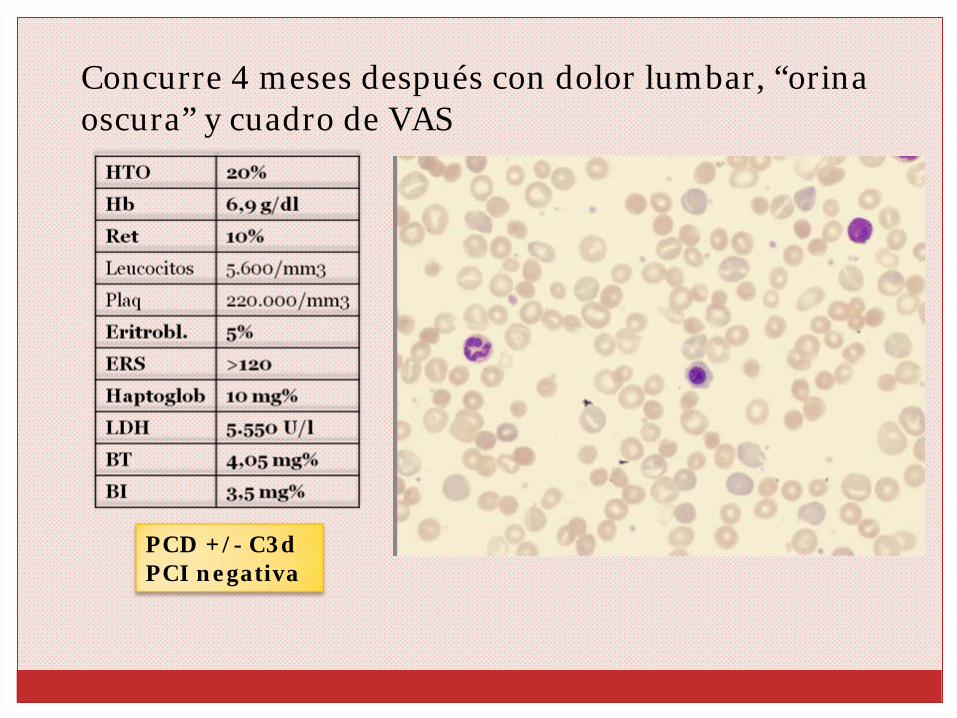
� Concurre 4 meses después con dolor lumbar, “orina oscura” y cuadro de VAS
PCD +/- C3dPCI negativa
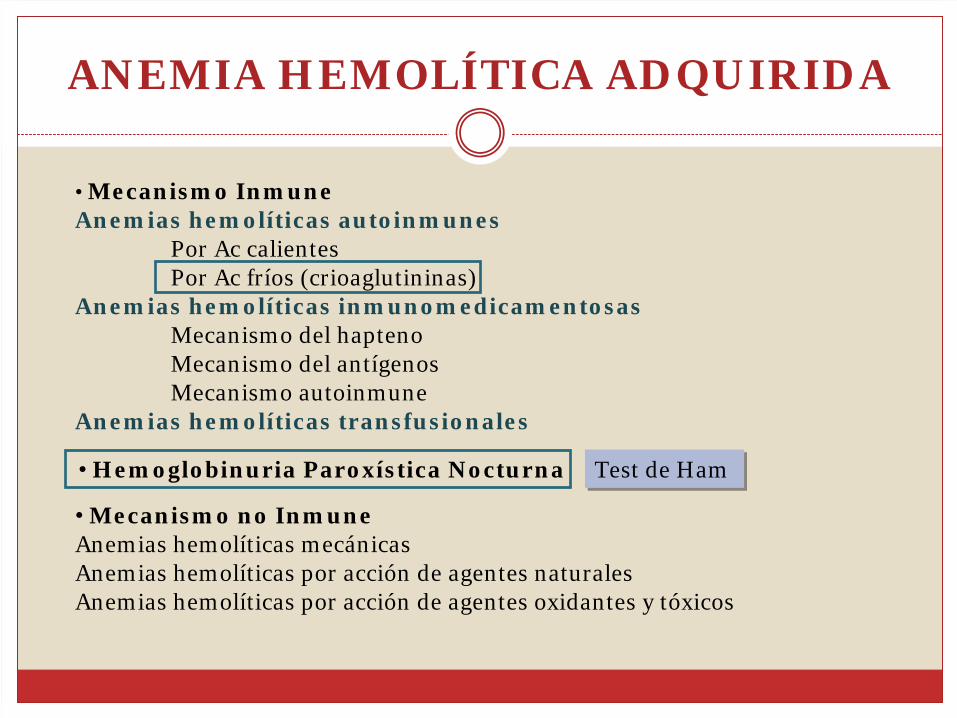
ANEMIA HEMOLÍTICA ADQUIRIDA
• Mecanismo InmuneAnemias hemolíticas autoinmunes
Por Ac calientesPor Ac fríos (crioaglutininas)
Anemias hemolíticas inmunomedicamentosasMecanismo del haptenoMecanismo del antígenosMecanismo autoinmune
Anemias hemolíticas transfusionales
Test de HamTest de Ham
• Mecanismo no Inmune Anemias hemolíticas mecánicasAnemias hemolíticas por acción de agentes naturalesAnemias hemolíticas por acción de agentes oxidantes y tóxicos
• Hemoglobinuria Paroxística Nocturna

ESTUDIOS COMPLEMENTARIOS
� Urocultivo negativo
� Ecografía abdomino-renal normal
� Serologías negativas
� Inmunológico: FAN, FR, Complemento s/p
� TAC tórax, abdomen y pelvis normal
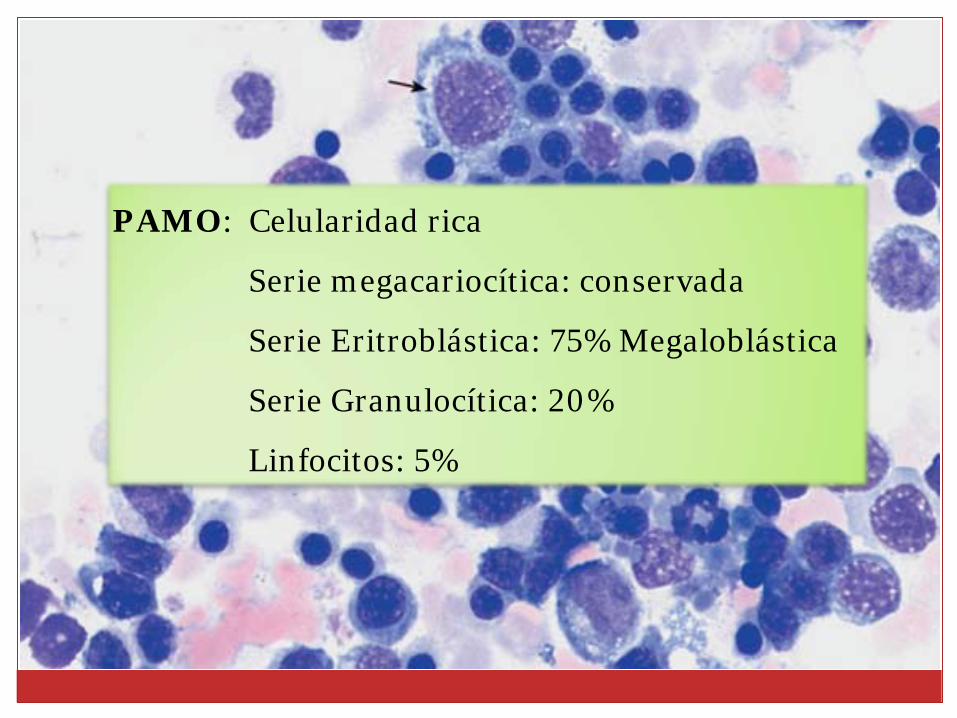
PAMO: Celularidad rica
Serie megacariocítica: conservada
Serie Eritroblástica: 75% Megaloblástica
Serie Granulocítica: 20%
Linfocitos: 5%

TRATAMIENTO
EVOLUCIÓN
03/2000
� Internación por crisis hemolítica
� Hto 23%, Hb 6,5 g/dl, Ret 3%, GB 1.700/mm3
(C2 S35 E4 L55 M4), Plaq 130.000/mm3, LDH
8.300 U/l
� Inmunohematológico negativo
� Test Ham negativo
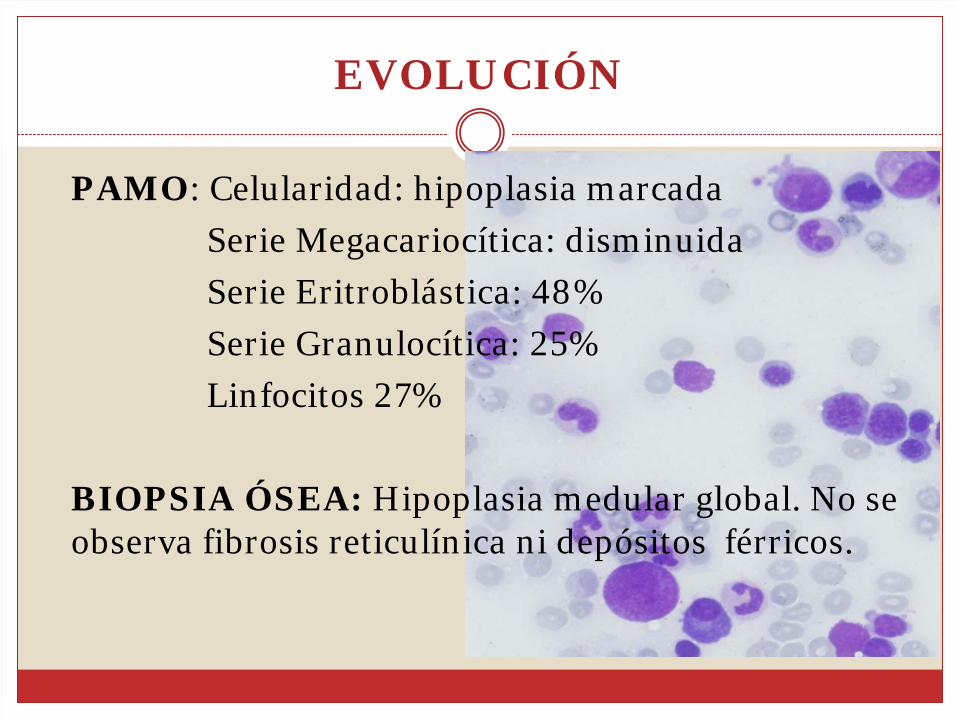
EVOLUCIÓN
� PAMO: Celularidad: hipoplasia marcada
Serie Megacariocítica: disminuida
Serie Eritroblástica: 48%
Serie Granulocítica: 25%
Linfocitos 27%
� BIOPSIA ÓSEA: Hipoplasia medular global. No se observa fibrosis reticulínica ni depósitos férricos.

EVOLUCIÓN
�Evolución estable
�Tratamiento con dosis bajas de prednisona
�Escaso requerimiento transfusional
�Algunos episodios de neutropenia febril
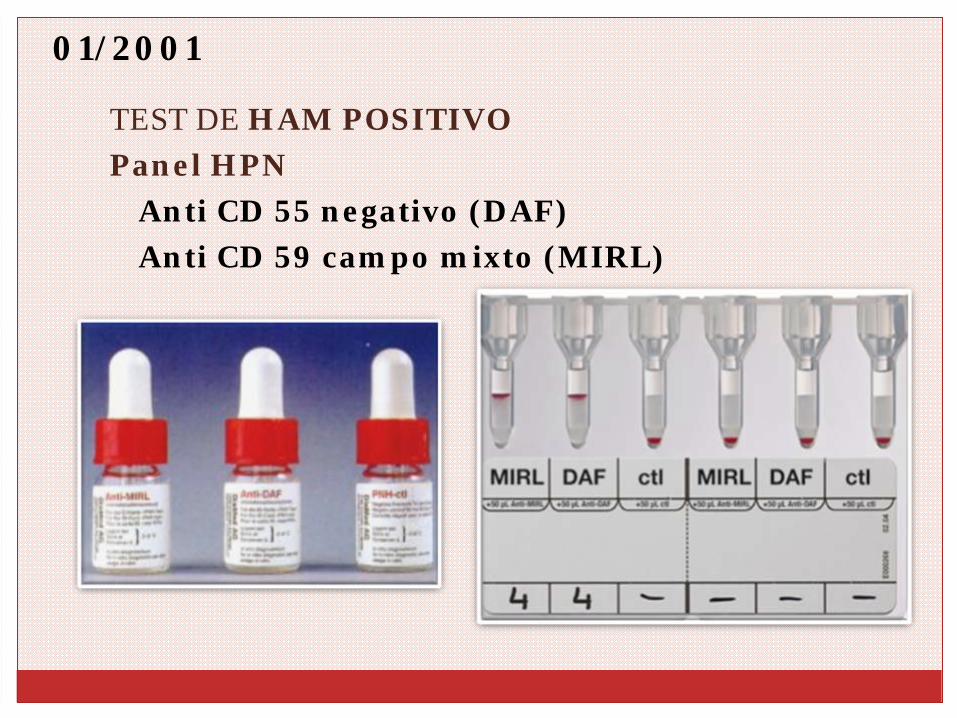
01/2001
� TEST DE HAM POSITIVO
� Panel HPN
� Anti CD 55 negativo (DAF)
� Anti CD 59 campo mixto (MIRL)

DIAGNÓSTICO
HEMOGLOBINURIA PAROXISTICA NOCTURNA

EVOLUCIÓN
Fiebre Dolor lumbarHemoglobinuria
TAC Abdominal Eco doppler eje esplenoportal sin evidencia de trombos
AngioRMN Normal
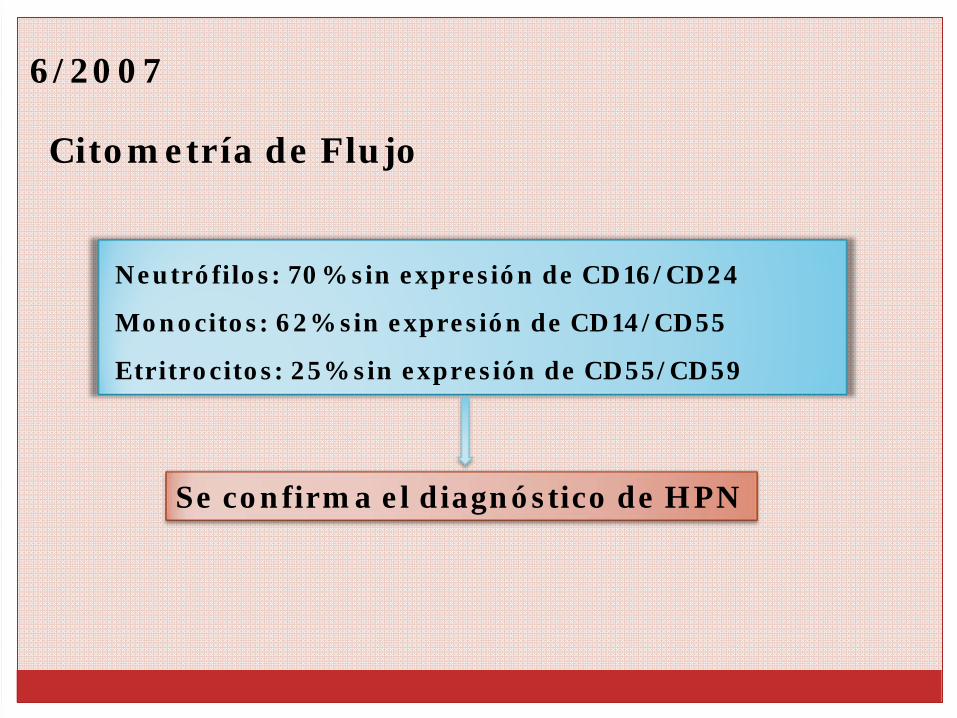
6/2007
Citometría de Flujo
Neutrófilos: 70% sin expresión de CD16/CD24
Monocitos: 62% sin expresión de CD14/CD55
Etritrocitos: 25% sin expresión de CD55/CD59
Se confirma el diagnóstico de HPN

EVOLUCIÓN
09/2008
� Dolor y asimetría en miembro inferior derecho
� Ecodoppler: TVP
� Anticoagulación con heparina sódica + acenocumarol
� Evolución favorable
Indicación de tratamiento con Eculizumab

EVOLUCIÓN
10/2008
� Internación por mal estado general, disnea, fiebre y
dolor abdominal intenso
� TAC abdomen y Ecodoppler normal
� Evolución desfavorable�Insuficiencia respiratoria
� ÓbitoHematológico: Hto: 34% Hb 11,9 g/dl, Ret 6,2%
Plaq 210.000/mm3 GB: 5200 (S72 E2 L24 M2)

HEMOGLOBINURIA PAROXISTICA NOCTURNA

HEMOGLOBINURIA PAROXISTICA NOCTURNA
§
Enfermedad clonal no maligna de la hemopoyesis
§
Poco frecuente: 1 a 10 casos/1.000.000 hab
§
Adulto joven
§
Caracterizada por
1) Hemólisis intravascular
2) ± fallo medular (citopenias)
3) ± trombosisParker C, et al. Blood 2005; 106: 3699‐3709

HEMOGLOBINURIA PAROXISTICA NOCTURNA
� Mutación somática adquirida del gen PIG-A (fosfatidil-inositol glucano A) a nivel de la célula madre hematopoyética
� Se transmite a toda su progenie: glóbulos rojos, glóbulos blancos y plaquetas del clon HPN
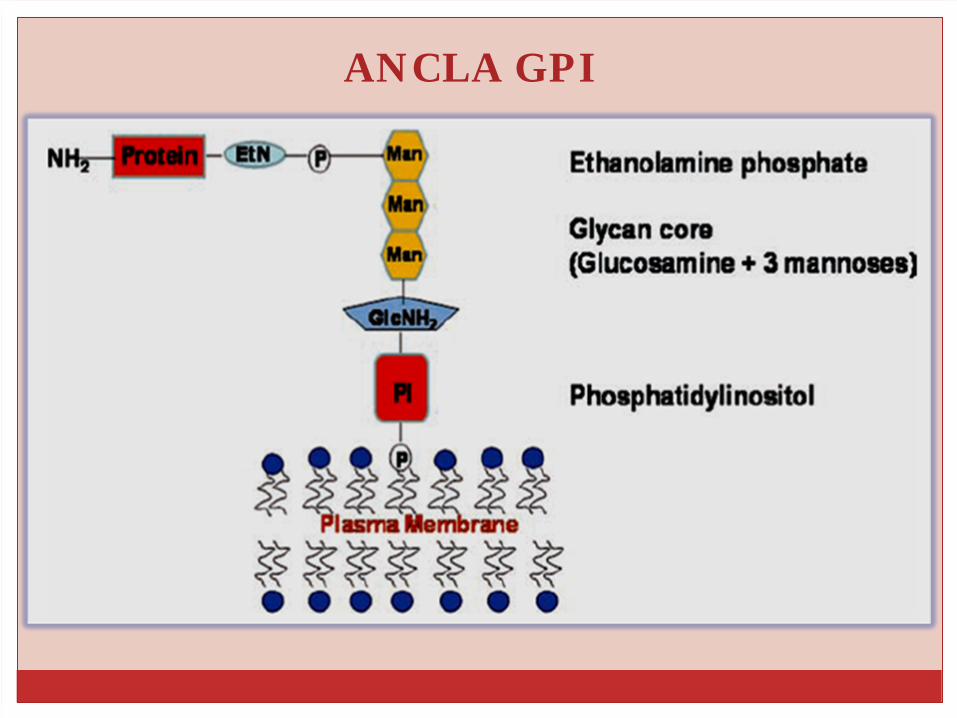
ANCLA GPI
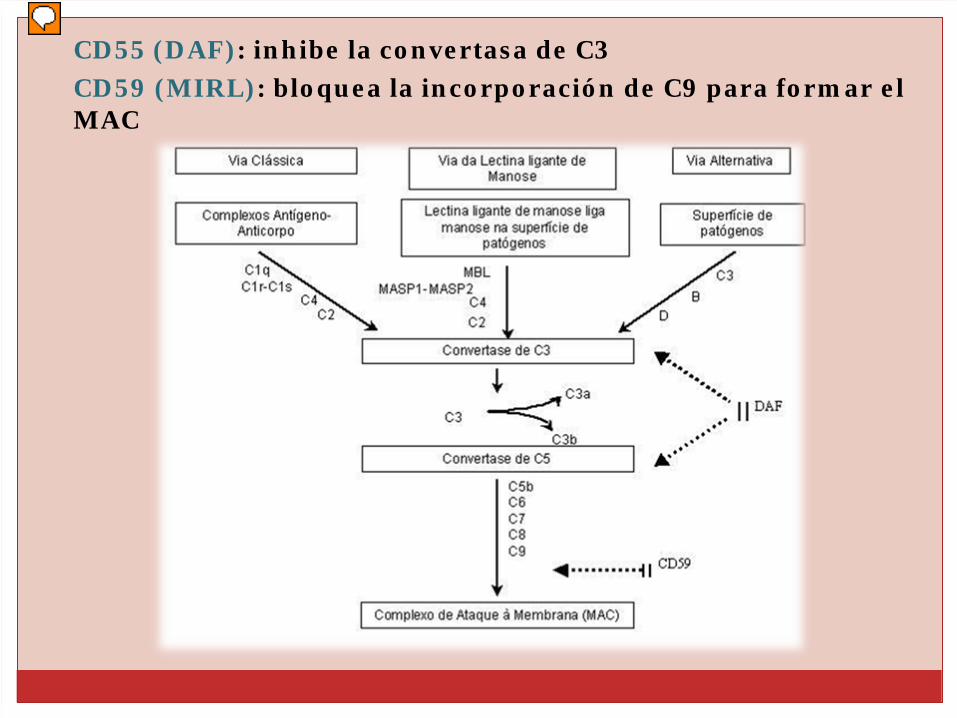
� CD55 (DAF): inhibe la convertasa de C3
� CD59 (MIRL): bloquea la incorporación de C9 para formar el MAC

HPNNORMAL C=O
Asp
C=O2 2
O
O=P=OO
O
CH CH CH
C=OO
CH2 CH2 NH
CH2CH2
NH
O2
O
O-P=O
O-P-OO
O
N
( 1-2)
( 1-6)
( 1-4)
PROTEIN
C=O
Asp
C=O
2
2
O
O=P=O
O
OCHCH
CHC=O
O
CH2 CH
2 NH
CH2CH
2
NH
O
2
OO-P=O
O-P-OO
O N
( 1-2)( 1-6)
( 1-4)
PROTEIN
GPI-anchor & membrane proteins
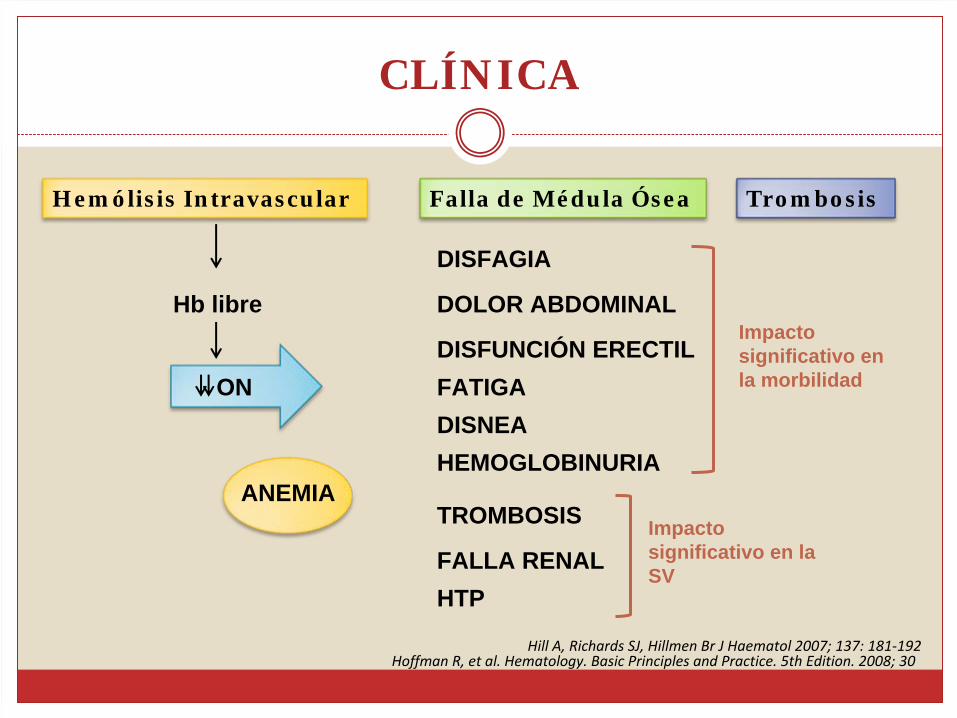
CLÍNICA
Hemólisis Intravascular
Hb libre
ANEMIA
TrombosisFalla de Médula Ósea
ON
TROMBOSIS
HTPFALLA RENAL
Impacto significativo en la SV
DOLOR ABDOMINAL
DISNEAFATIGA
DISFAGIA
HEMOGLOBINURIA
DISFUNCIÓN ERECTILImpacto significativo en la morbilidad
Hill A, Richards SJ, Hillmen Br J Haematol 2007; 137: 181‐192Hoffman R, et al. Hematology. Basic Principles and Practice. 5th
Edition. 2008; 30

CLASIFICACIÓN
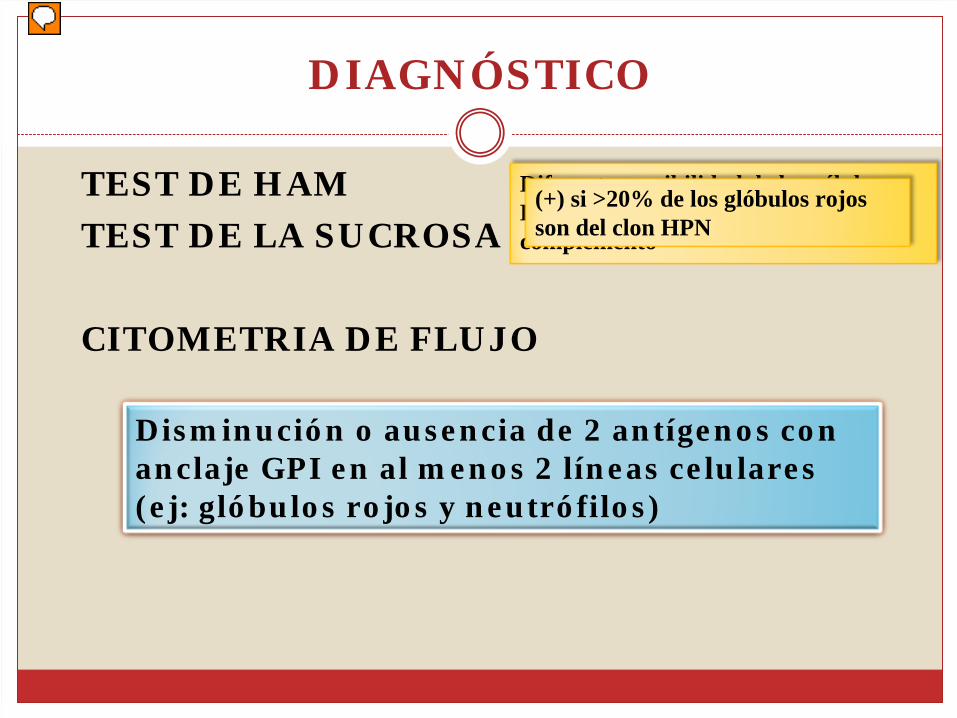
DIAGNÓSTICO
� TEST DE HAM
� TEST DE LA SUCROSA
� CITOMETRIA DE FLUJO
HISTÓRICODiferente sensibilidad de las células HPN y normales a la acción del complemento
•Sensible y específico•Tamaño clon •El resultado se afecta menos por las transfusiones
(+) si >20% de los glóbulos rojos son del clon HPN
Disminución o ausencia de 2 antígenos con anclaje GPI en al menos 2 líneas celulares (ej: glóbulos rojos y neutrófilos)
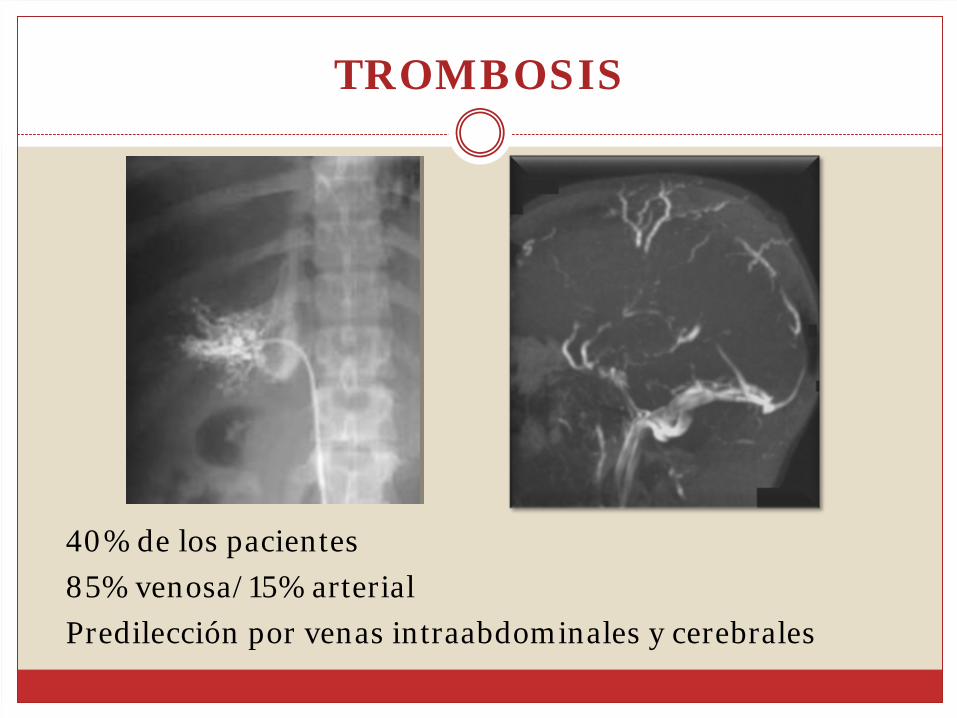
TROMBOSIS
� 40% de los pacientes
� 85% venosa/15% arterial
� Predilección por venas intraabdominales y cerebrales

TROMBOSIS
Hillmen et al.
Blood 2007; 110: 4123-4128 International PNH Group et al. Blood. 2005

TROMBOSIS: MECANISMOS
§ ↓TFPI en membrana por falta de chaperona con ancla GPI
üAumento de la agregación y adhesión plaquetariaüFormación del coágulo acelerada
§
Plaquetas HPN: Formación de microvesículas y externalización de fosfatidilserina (procoagulante in vitro)
§ Alteración de la fibrinolisis
§
Activación leucocitaria (neutrófilos y monocitos HPN) por complemento y ↑
C5a → inflamación y expresión de F. tisular
§ Disfunción endotelial→ daño por complemento
Hill A et al. Br J Haematol. 2007;137:181-192 Weitz I et al. Blood. 2008; 112: Abstract 407Maroney SA et al J Thromb Haemost 2006;4:1114-24
§ Disminución de ON

TRATAMIENTO
• Tasa de respuesta > 50%•
Globulina antitimocítica y/o
ciclosporina• Clon HPN no se ve afectado •
No beneficia a pacientes con
HPN clásica

ECULIZUMAB
•
Anticuerpo monoclonal humanizado Ig G kappa
•
Se une específicamente a la proteína C5, inhibiendo la activación del complemento terminal
•
Primera droga efectiva en el tratamiento de la HPN
•
Fue aprobada por la FDA en 2007
Brodsky R. Blood 2009; 113: 6522-6527

ECULIZUMAB
Hillman P, et al. Blood 2007; 110 (12): 4123‐4128Roth A, Duhrsen U. European Journal of Hematology 2011; 87: 473‐479
Kelly, R, et.al. Blood 2011; 117(25): 6786‐6792

ECULIZUMAB: INDICACIONES
Roth A, Duhrsen U. European Journal of Hematology 2011; 87: 473‐479
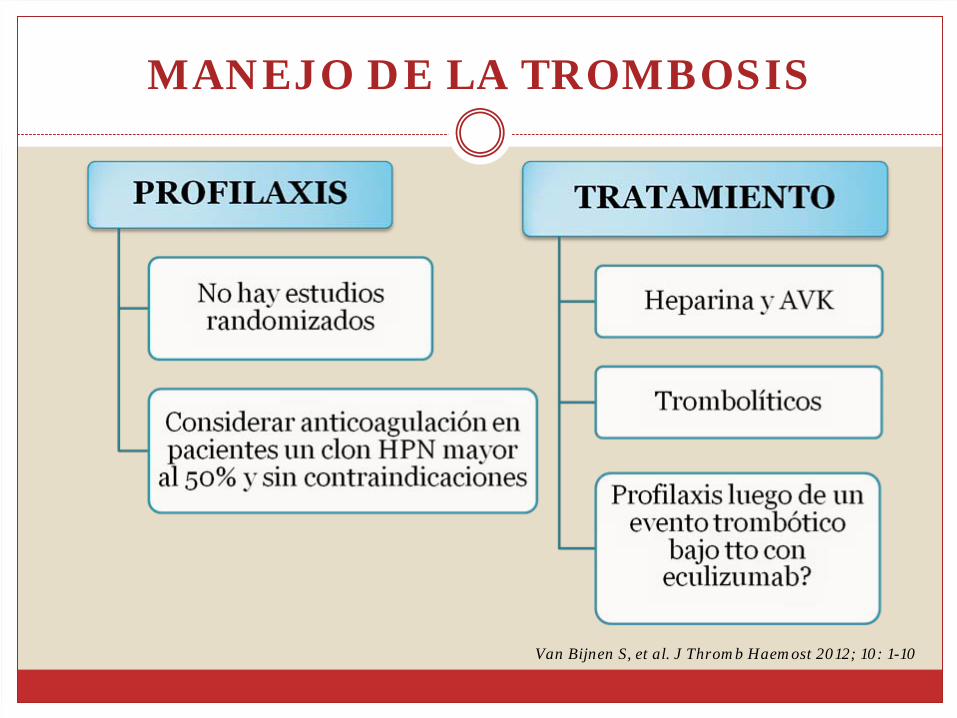
MANEJO DE LA TROMBOSIS
Van Bijnen S, et al. J Thromb Haemost 2012; 10: 1-10

TRASPLANTE ALOGÉNICO DE PRECURSORES HEMATOPOYÉTICOS
� Único tratamiento curativo
� Morbimortalidad significativa
INDICACIONES
Therapeutics and Clinical Risk Management 2009;5:911


BIBLIOGRAFÍA
� Hill A, Richards S, Hillmen P. Recents developments in the understanding and managment of paroxysmal nocturnal hemoglobinuria. BJH (2007), 137: 181- 192.
� Van Bijnen S, Van Heerde W, Muus P. Mechanisms and clinical implications of thrombosis in paroxysmal nocturnal hemoglobinuria. J Thromb Haemost 2012; 10: 1-10.
� Brodsky R. How I treat paroxysmal nocturnal hemoglobinuria. Blood 2009; 113: 6522-6527.
� Luzzatto L, Gianfaldoni G, Notaro R. Managment of paroxysmal nocturnal hemoglobinuria: a personal view. BJH 2011; 153: 709-720.
� Roth A, Duhrsen U. Treatment of paroxysmal nocturnal hemoglobinuria in the era of eculizumab. European Journal of Hematology 2011; 87: 473-479.
� Hoffman R, Benz E, Shattil S, et al. Hematology. Basic Principles and Practice. 5th Edition. Churchil Livingstone. 2008; 30.

Muchas Gracias!!