secuenciaciÓn de la hormonoterapia en la … · repaso histÓrico. secuencia Óptima del...
TRANSCRIPT

SECUENCIACIÓN DE LA HORMONOTERAPIA EN LA
ENFERMEDAD METASTÁSICA.
REPASO HISTÓRICO
Lourdes CalvoComplejo Hospitalario Universitario A Coruña
• Evolución histórica de la HT
• Cirugía ablativa
• Fármacos hormonales
• (Otras terapias dirigidas)
• Secuenciación de la Hormonoterapia
SECUENCIACIÓ DE LA HORMONOTERAPIA EN CMM REPASO
HISTÓRICO
TIMER
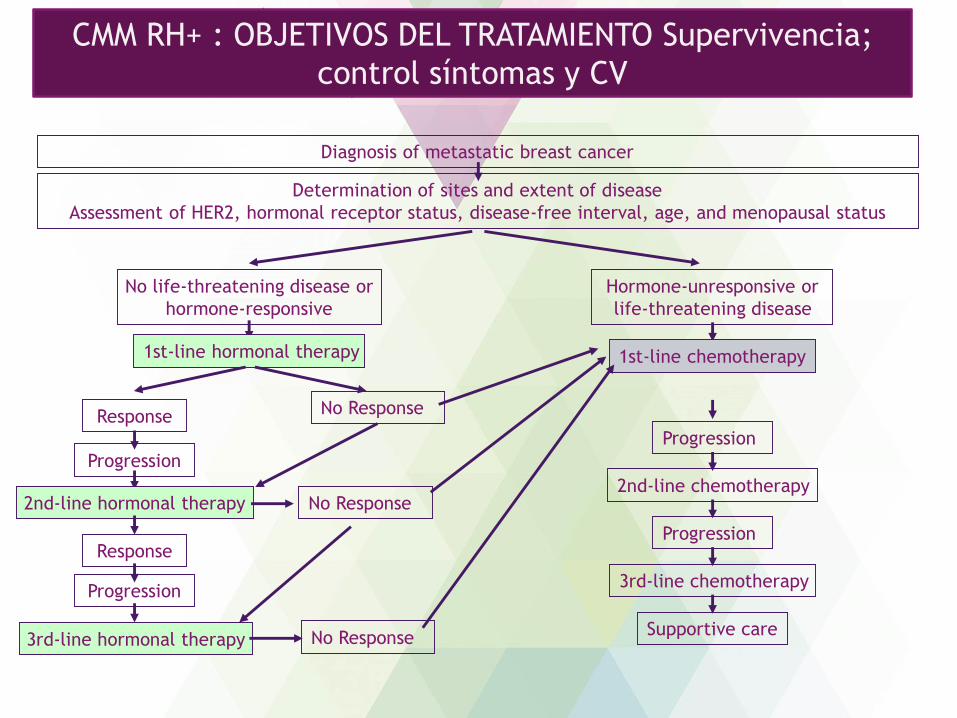
Diagnosis of metastatic breast cancer
Determination of sites and extent of disease
Assessment of HER2, hormonal receptor status, disease-free interval, age, and menopausal status
No life-threatening disease or
hormone-responsive
Hormone-unresponsive or
life-threatening disease
1st-line hormonal therapy 1st-line chemotherapy
Response No Response
2nd-line hormonal therapy2nd-line chemotherapy
Progression
Progression
Progression
Progression
3rd-line hormonal therapy
Response
No Response
No Response
3rd-line chemotherapy
Supportive care
CMM RH+ : OBJETIVOS DEL TRATAMIENTO
Supervivencia; control síntomas y CVCMM RH+ : OBJETIVOS DEL TRATAMIENTO Supervivencia;
control síntomas y CV

Diagnosis of metastatic breast cancer
Determination of sites and extent of disease
Assessment of HER2, hormonal receptor status, disease-free interval, age, and menopausal status
No life-threatening disease or
hormone-responsive
Hormone-unresponsive or
life-threatening disease
1st-line hormonal therapy 1st-line chemotherapy
Response No Response
2nd-line hormonal therapy2nd-line chemotherapy
Progression
Progression
Progression
Progression
3rd-line hormonal therapy
Response
No Response
No Response
3rd-line chemotherapy
Supportive care
mPFS: 12-15m
mPFS: 3-4 m
Varias líneas de HT Resistencia
Respuesta a 1ª L HT predice la respuesta a otras líneas.
CMM RH+ : OBJETIVOS DEL TRATAMIENTO Supervivencia;
control síntomas y CV
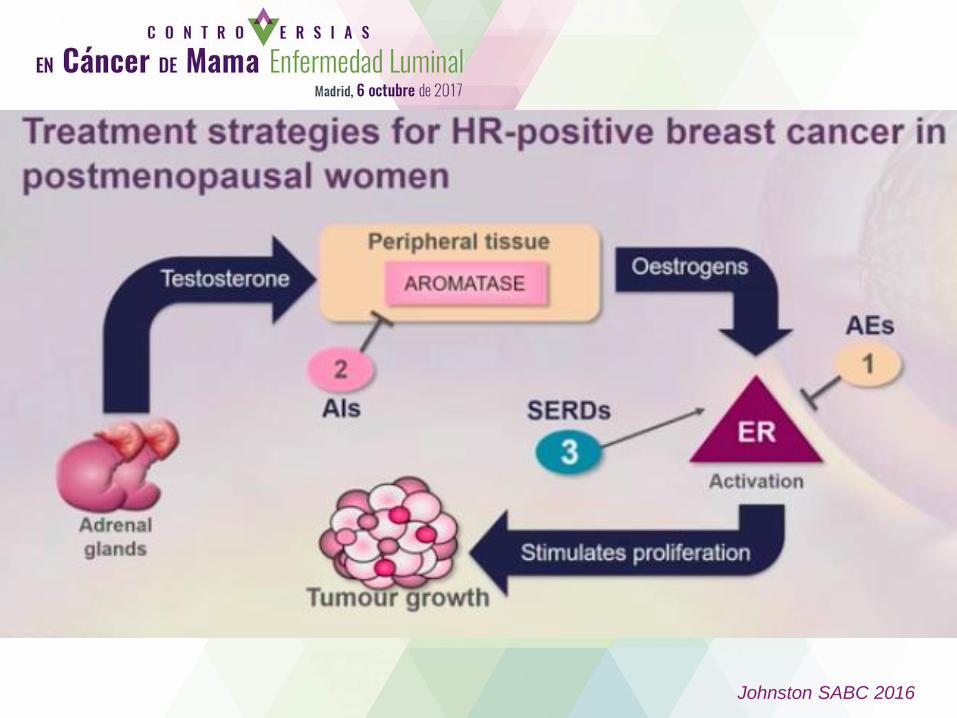
Johnston SABC 2016
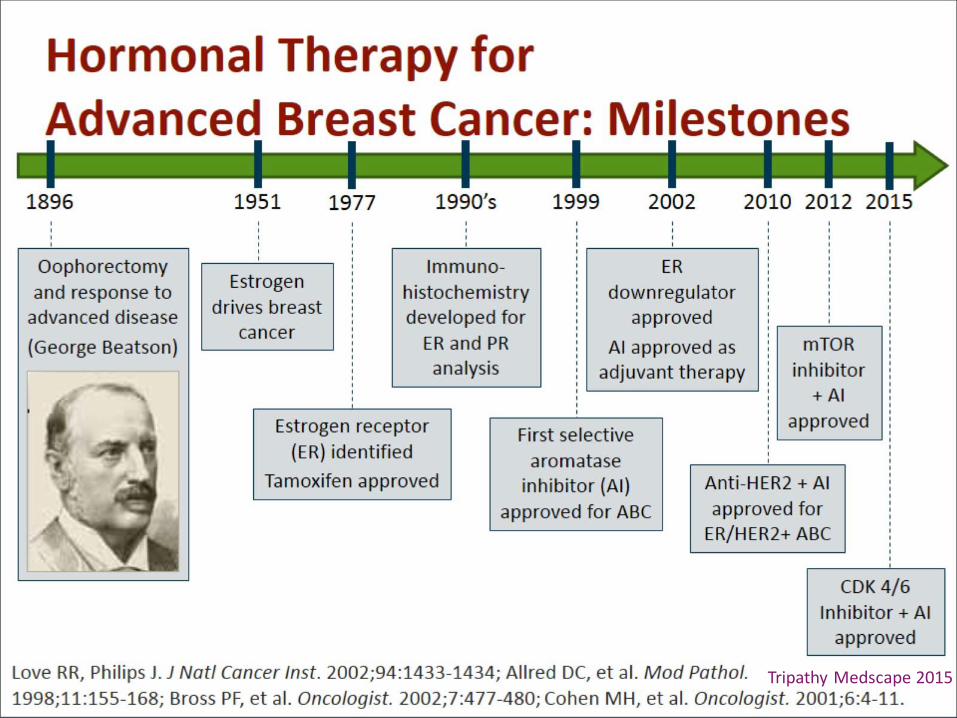
Tripathy Medscape 2015
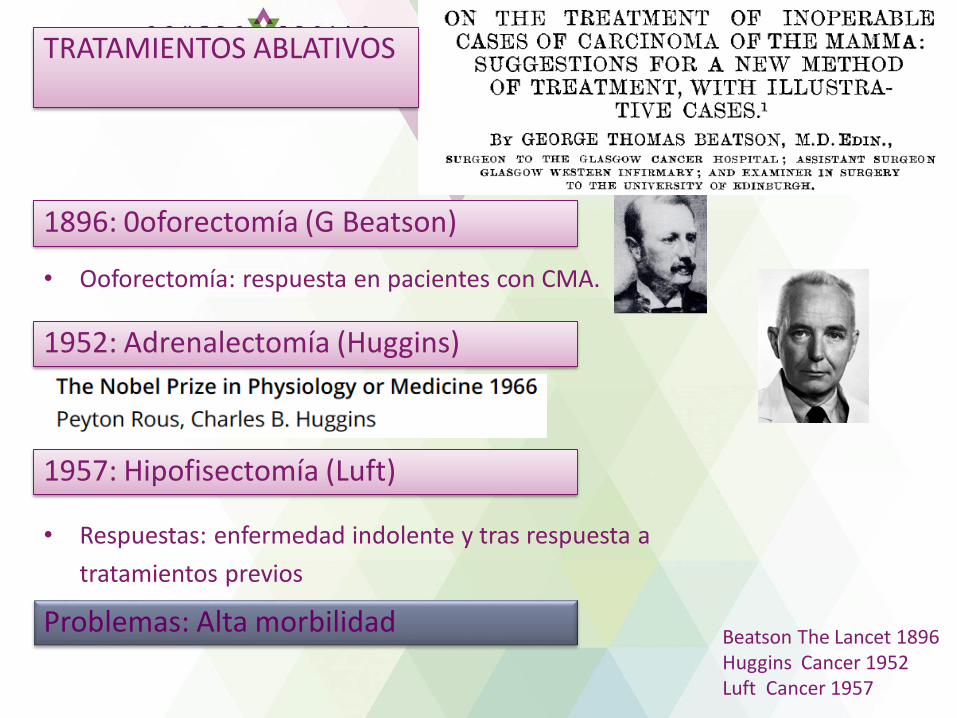
• Ooforectomía: respuesta en pacientes con CMA.
1896: 0oforectomía (G Beatson)
Beatson The Lancet 1896Huggins Cancer 1952Luft Cancer 1957
1952: Adrenalectomía (Huggins)
1957: Hipofisectomía (Luft)
TRATAMIENTOS ABLATIVOS
• Respuestas: enfermedad indolente y tras respuesta a
tratamientos previos
Problemas: Alta morbilidad
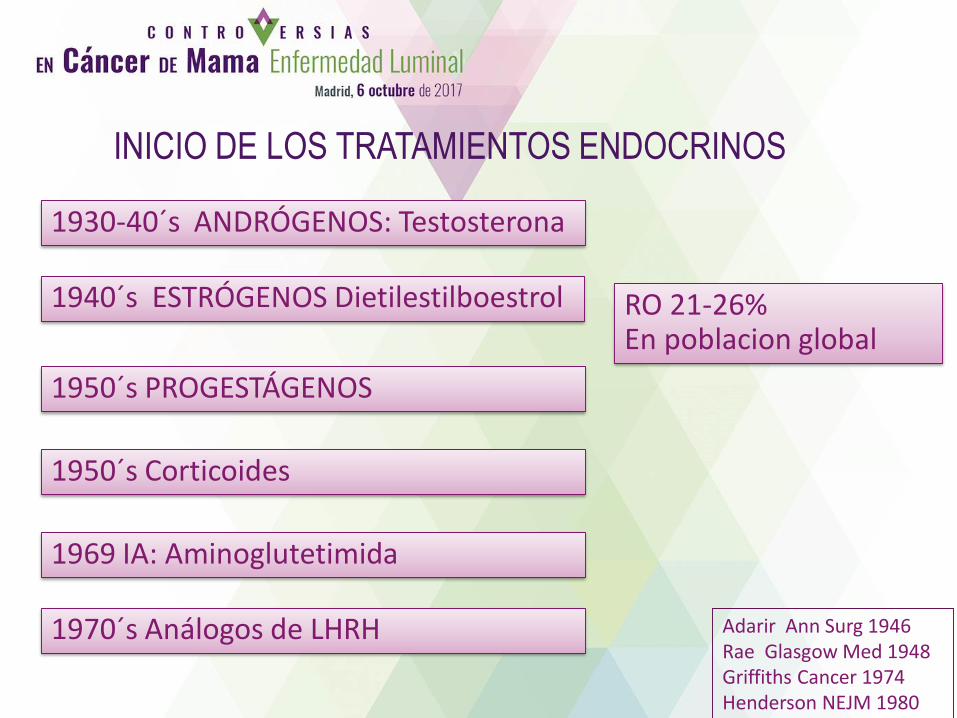
1930-40´s ANDRÓGENOS: Testosterona
INICIO DE LOS TRATAMIENTOS ENDOCRINOS
1969 IA: Aminoglutetimida
1950´s PROGESTÁGENOS
1940´s ESTRÓGENOS Dietilestilboestrol
Adarir Ann Surg 1946Rae Glasgow Med 1948Griffiths Cancer 1974Henderson NEJM 1980
1950´s Corticoides
1970´s Análogos de LHRH
RO 21-26%En poblacion global

• Descripción de RH en el tejido tumoral de cáncer de mama.
• Valor predictivo de respuesta a los tratamientos hormonales: Relación de
la expresión de RH y respuesta a adrenalectomía y otros.
• Variabilidad en la expresión de RH dentro del mismo tumor y en las
distintas localizaciones metastásicas.
23/2/15 18:46Elwood Jensen, molecular b iologist , d ies at 92 - Chicago T ribune
Pág ina 1 de 6ht tp:/ /art ic les.chicagotribune. com/2012-12-24/news/ct -met-elwo…nsen-obit -20121224_1_elwood- jensen- tamoxifen-estr ogen- receptor
0RecomendarRecomendar 0
0
Elwood Jensen, 1920 -20 12M olecular biologist whose work allowed
breast cancer to be treated with tamoxifen
December 24, 2012 | By Graydon Megan, Special to the
Tribune
Molecular biologist Elwood Jensen was a pioneering
cancer researcher whose work in the 1980s on
techniques for detecting and measuring estrogen
receptors in breast cancer still provides guidance for
treatment of the disease.
"His work changed the way all breast cancers are
analyzed," said Geoffrey Greene, who worked with
Mr. Jensen in what is now the Ben May Department
for Cancer Research at the University of Chicago,
where Mr. Jensen was the Charles B. Huggins
distinguished service professor emeritus.
Related Ar ticles
A Coruña - Madrid€43.37
¡Reserva Online en
Iberia.com!
Iberia
(http://www.trbimg.com/img-Elwood Jensen (handout, HANDOUT)
Prestigious Lasker
Award goes to U. of C.
researcher (/2004-09-
26/news/0409260326_1_lasker-
awards-breast-cancer-
hormones)
September 26, 2004
Extra pounds tied to
breast cancer
131
(http://www.chicagotribune.com)
HOME (HTTP://WWW.CHICAGOTRIBUNE.COM) NEWS (HTTP://WWW.CHICAGOTRIBUNE.COM/NEWS/)
BUSINESS (HTTP://WWW.CHICAGOTRIBUNE.COM/BUSINESS/)
SPORTS (HTTP://WWW.CHICAGOTRIBUNE.COM/SPORTS/)
A&E (HTTP://WWW.CHICAGOTRIBUNE.COM/ENTERTAINMENT/)
LIFESTYLES (HTTP://WWW.CHICAGOTRIBUNE.COM/FEATURES/)
OPINION (HTTP://WWW.CHICAGOTRIBUNE.COM/NEWS/OPINION/)
REAL ESTATE (HTTP://WWW.CHICAGOTRIBUNE.COM/CLASSIFIED/REALESTATE/)
CARS (HTTP://WWW.CHICAGOTRIBUNE.COM/CLASSIFIED/AUTOMOTIVE/)
JOBS (HTTP://WWW.CHICAGOTRIBUNE.COM/CLASSIFIED/JOBS/)1962 Jensen: RE
Jensesn 1967Mass AJOG 1972Engelsman BMJ 1973
1973 DILEMA: ¿Realizar cirugía ablativa en las pacientes sin conocer el estado de los RH?

• 1960´s como anticonceptivo…
• Actividad antitumoral en estudios preclínicos
• Aprobado por la FDA en 1977
• En pre-menopáusicas igual eficacia que AO.
• Comparado con HT previas en ECA no diferencias
en respuestas pero menor toxicidad.
• Meta-análisis confirma no diferencias en RO ni
SV pero mejor tolerancia del TMX.
Jordan LanOncol 2000
Fossati JCO 1998
TAMOXIFENO 1967 _ ICI-46, 474AL Walpole, VC Jordan
TAMOXIFENO: estándar en 1ª L CMM 1970-2000
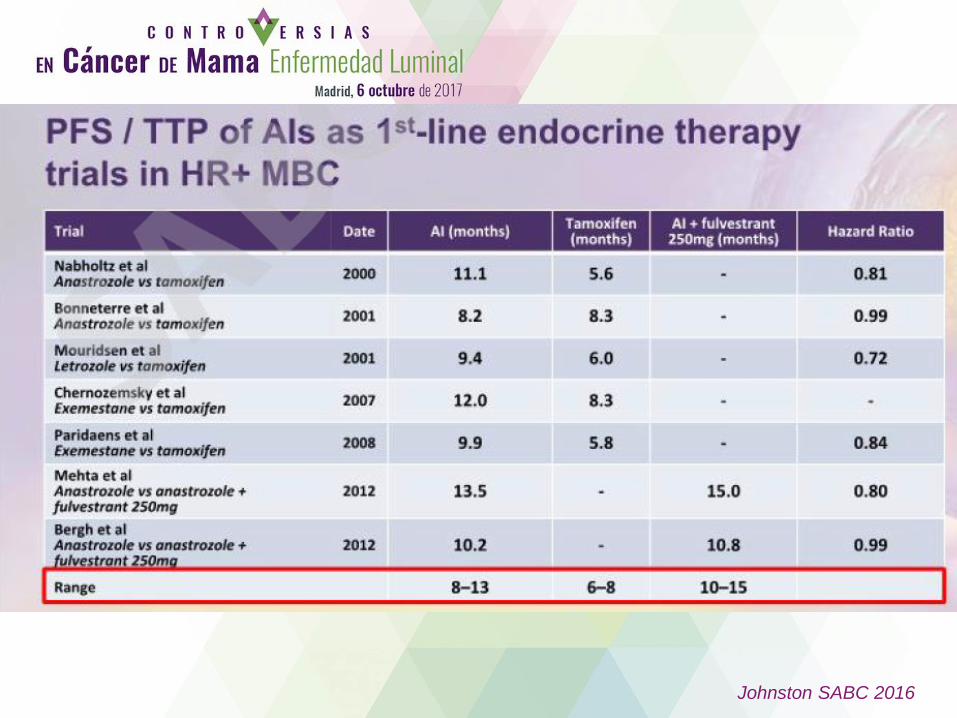
Johnston SABC 2016

I Álvarez Rev Cáncer 2017

• FULVESTRANT 250 vs EXEMESTANO (EFFECT)
• No diferencias en TP
• FULVESTRANT 250 + ANAST vs FULV-PLACEBO vs EXEMESTANO
(SOFEA)
• No diferencias en TP ni en SG.
• FULVESTRANT 500 vs 250 (CONFIRM)
• F 500: > TP (6.5 vs 5.5 m) y > SG (26.4 vs 22.3 m).
Buzdar JCO 2001; Buzdar Cancer 1998; Kaufman JCO 2000; Robertson Cancer 2003;
Chia JCO 2008; Johnston Lancet Oncol 2013; Di Leo JNCI 2014
HORMONOTERAPIA CMM: RESULTADOS EC 2ªL CMM FASE III TRAS PROG A IA
HORMONOTERAPIA CMM: RESULTADOS EC 2ªL CMM FASE III TRAS PROG A SERMs
• IA 3ª GENERACIÓN FRENTE A ACETATO DE MEGESTROL
• No diferencias en TP para Letrozol o Anastrozol.
• Exemestano > TP y > SG que AM.• IA menos efectos secundarios
• FULVESTRANT 250 vs ANASTROZOL
• No diferencias en TP ni en SG.

Johnston SABC 2016

TRATAMIENTOS APROBADOS PARA EL CMM RH+
Modificado de Chlebowski 2013
Palbociclib
FDA (2015)
2015
Ribociclib
FDA (2017)
2017

TÍTULO
1960´s 1970’s 1990´s 2000´s
I Estrógenos
II ProgestágenosAndrógenosCorticoides
III Adrenalectomía
Hipofisectomía
I Tamoxifeno
II Megestrol
Aminoglute-
timida
III Estrógenos
I IA 3ª generac.
II-III Fulvestrant ó
IA sin R cruzada ó
Tamoxifeno
IV Megestrol
Estrógenos
I Tamoxifeno
II IA 3ª generac.
III Exemestano
Megestrol
Estrógenos
Al Nivel 1 de evidencia
Post Al > incertidumbre
SECUENCIA DEL TRATAMIENTO HORMONAL
REPASO HISTÓRICO

SECUENCIA ÓPTIMA DEL TRATAMIENTO ENDOCRINO EN CMM
RH+ HER2-
• Desde el 2000 el estándar en 1ª L de CMM han sido los IA.
• Con la incorporación de los nuevos fármacos obtenemos
mejores resultados y aumentan las controversias de
cómo elegir el tratamiento más adecuado.
• 1ª línea
– PFS de 14-16 meses con IA o Fulvestrant
– Combinaciones con Inhibidores de CDK 4/6: PFS > 24 meses
– ¿Cómo seleccionar a las pacientes?
– ¿Què pacientes podemos tratar solo con HT?
CUESTIONES PENDIENTES
SECUENCIA DEL TRATAMIENTO DEL CMM RH+ HER2-

• 2ª Línea
– Combinaciones de HT: PFS de 7-9 meses
– ¿Qué tratamientos utilizaremos tras progresión a ICDK?
• ¿Cómo elegir la secuencia?
– Biología tumoral, características y preferencias de las pacientes
• Necesitamos factores predictores que nos ayuden a
seleccionar el mejor tratamiento para cada paciente.
CUESTIONES PENDIENTES
SECUENCIA DEL TRATAMIENTO DEL CMM RH+ HER2-
MUCHAS GRACIAS