anances en diagnÓstico - geicam.org · dr. vicente martínez de vega hospital quirón madrid ....
TRANSCRIPT
ANANCES EN DIAGNÓSTICO Dr. Vicente Martínez de Vega
Hospital Quirón Madrid
METODOS DIAGNÓSTICOS
• Resonancia Magnética
•Mamografía (Tomosíntesis) • Ecografía
• PET-TAC
RESONANCIA MAGNÉTICA DE MAMA
• RM de mama y Cirugía del cáncer de mama
• RM de mama y Difusión
• RM de mama y Ecografía second-look
• RM de mama y Cribado en pacientes de alto riesgo
• RM de mama y Quimioterapia neoadyuvante
• RM de mama y Papilomas
• RM de mama y Caracterización de lesiones
• RM de mama y Tamaño tumoral
Aproximadamente 800 artículos publicados (Junio 2014- Junio 2015)
RM DE MAMA Y CIRUGÍA
Br J Surg. 2015 Apr 28. doi: 10.1002/bjs.9797. [Epub ahead of print]
Meta-analysis of the effect of preoperative breast MRI on the surgical
management of ductal carcinoma in situ.
Fancellu A1, Turner RM, Dixon JM, Pinna A, Cottu P, Houssami N.
RESULTS:
Nine eligible studies were identified that included 1077 women with DCIS who
had preoperative MRI and 2175 who did not. MRI significantly increased the
odds of having initial mastectomy (OR 1·72, P = 0·012; adjusted OR 1·76,
P = 0·010). There were no significant differences in the proportion of
women with positive margins following breast-conserving surgery (BCS) in
the MRI and no-MRI groups (OR 0·80, P = 0·059; adjusted OR 1·10, P = 0·716),
nor in the necessity of reoperation for positive margins after BCS (OR 1·06,
P = 0·759; adjusted OR 1·04, P = 0·844). Overall mastectomy rates did not differ
significantly according to whether or not MRI was performed (OR 1·23,
P = 0·340; adjusted OR 0·97, P = 0·881).
CONCLUSION:
Preoperative MRI in women with DCIS is not associated with improvement
in surgical outcomes.
RM DE MAMA Y CIRUGÍA
Br J Surg. 2015 Apr 28. doi: 10.1002/bjs.9797. [Epub ahead of print]
Meta-analysis of the effect of preoperative breast MRI on the surgical
management of ductal carcinoma in situ.
CONCLUSION:
Preoperative MRI in women with DCIS is not associated with improvement in
surgical outcomes.
La RM se utiliza para estudio preoperatorio
pero no para marcar prequirúrgicamente

Vicente Martinez De Vega, MD; S Linares Gonzalez, MD; J Oyola Tovar, MD; D C Mollinedo, MD; L Alvarez Perez, BMedSc; M Chiva De Agustin MD; Manuel Recio Rodríguez MD ([email protected])
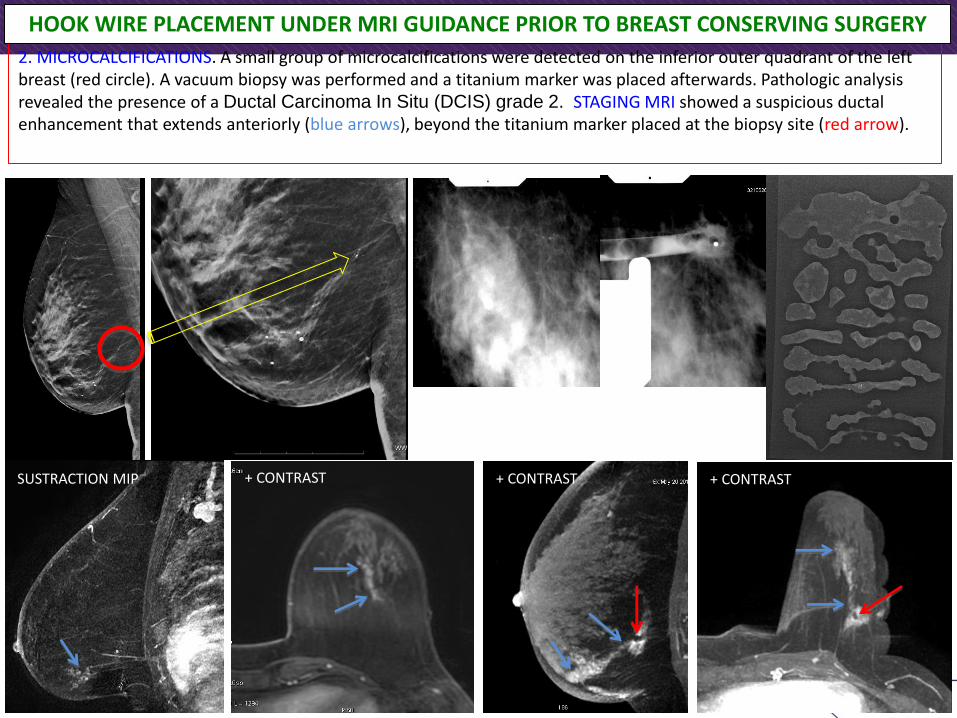
2. MICROCALCIFICATIONS. A small group of microcalcifications were detected on the inferior outer quadrant of the left breast (red circle). A vacuum biopsy was performed and a titanium marker was placed afterwards. Pathologic analysis revealed the presence of a Ductal Carcinoma In Situ (DCIS) grade 2. STAGING MRI showed a suspicious ductal enhancement that extends anteriorly (blue arrows), beyond the titanium marker placed at the biopsy site (red arrow).
SUSTRACTION MIP + CONTRAST + CONTRAST + CONTRAST
HOOK WIRE PLACEMENT UNDER MRI GUIDANCE PRIOR TO BREAST CONSERVING SURGERY
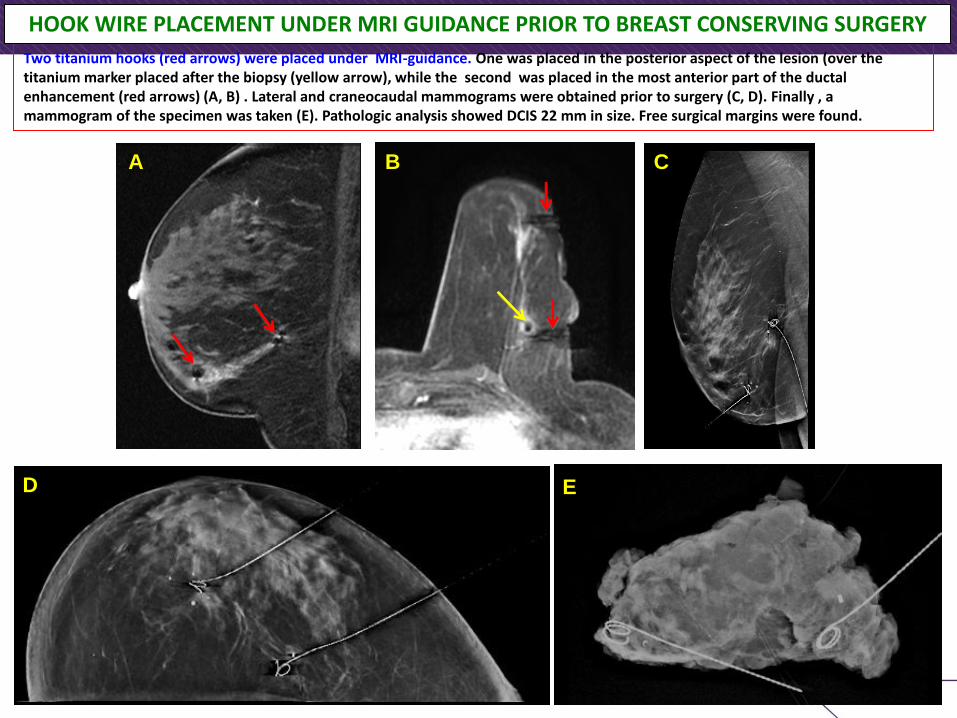
Two titanium hooks (red arrows) were placed under MRI-guidance. One was placed in the posterior aspect of the lesion (over the titanium marker placed after the biopsy (yellow arrow), while the second was placed in the most anterior part of the ductal enhancement (red arrows) (A, B) . Lateral and craneocaudal mammograms were obtained prior to surgery (C, D). Finally , a mammogram of the specimen was taken (E). Pathologic analysis showed DCIS 22 mm in size. Free surgical margins were found.
HOOK WIRE PLACEMENT UNDER MRI GUIDANCE PRIOR TO BREAST CONSERVING SURGERY
A B C
D E
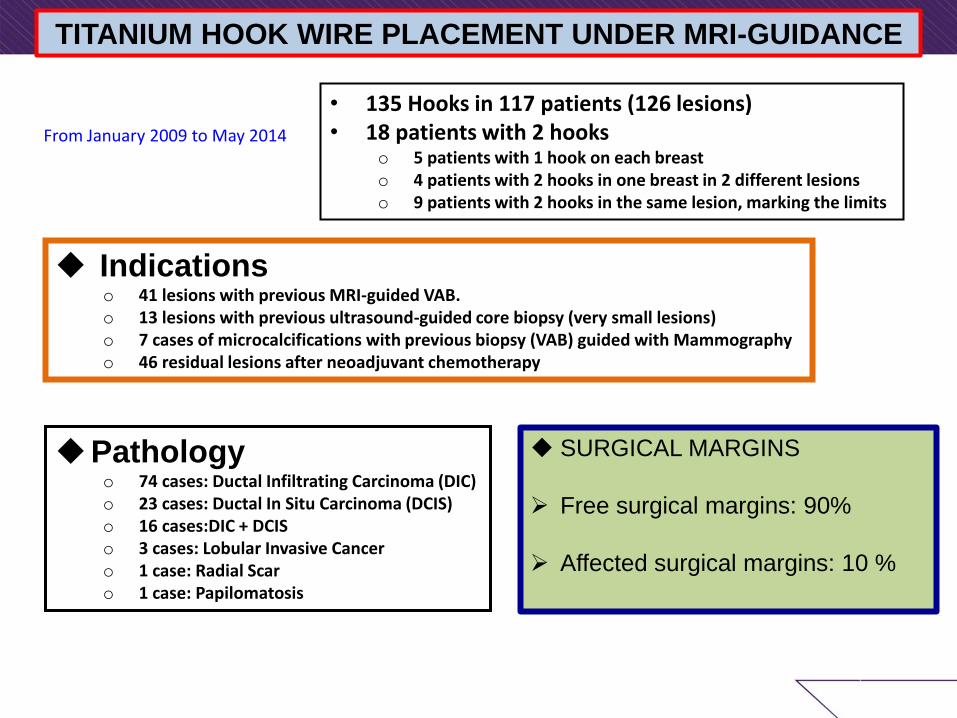
TITANIUM HOOK WIRE PLACEMENT UNDER MRI-GUIDANCE
• 135 Hooks in 117 patients (126 lesions) • 18 patients with 2 hooks
o 5 patients with 1 hook on each breast o 4 patients with 2 hooks in one breast in 2 different lesions o 9 patients with 2 hooks in the same lesion, marking the limits
Indications o 41 lesions with previous MRI-guided VAB. o 13 lesions with previous ultrasound-guided core biopsy (very small lesions) o 7 cases of microcalcifications with previous biopsy (VAB) guided with Mammography o 46 residual lesions after neoadjuvant chemotherapy
Pathology o 74 cases: Ductal Infiltrating Carcinoma (DIC) o 23 cases: Ductal In Situ Carcinoma (DCIS) o 16 cases:DIC + DCIS o 3 cases: Lobular Invasive Cancer o 1 case: Radial Scar o 1 case: Papilomatosis
From January 2009 to May 2014
SURGICAL MARGINS
Free surgical margins: 90%
Affected surgical margins: 10 %
RM DE MAMA Y CIRUGÍA: ROLL-SNOLL World J Surg Oncol. 2014 Oct 23;12:320. doi: 10.1186/1477-7819-12-320.
Magnetic resonance imaging-guided occult breast lesion localization and simultaneous
sentinel lymph node mapping. de Lima Docema MF, Costa PA, de Andrade FE, Bevilacqua JL, Elias S1, Cerri GG, Barros AC, Nazario AC.
METHODS:
This is a descriptive study of data collected retrospectively. Pre-operative mapping of 34 breast lesions
in 25 patients suspected of being malignant was performed using conventional imaging methods with a
magnetic resonance imaging-guided radiopharmaceutical injection.
RESULTS:
The mean time required to perform the localization was 25 minutes. After resection of the lesions using
a gamma probe, malignancy was confirmed in fifteen patients (60.0%), with nine invasive ductal
carcinomas, two invasive lobular carcinomas, and four in situ ductal carcinomas The resection was
confirmed by the complete removal of the radioactive material. The pathologic results and images were
concordant in all but two cases, which were submitted for new magnetic resonance imaging
examinations and surgery that confirmed the malignancies. Of the 15 patients with confirmed
malignancies, 10 had sentinel lymph node resection. Of these, eight were negative for metastases, one
had micro-metastases and one had confirmed metastases. Three patients had full axillary node
dissection, with metastases found in only one. No side effects were observed with magnetic resonance-
guided radiopharmaceutical injection.
CONCLUSIONS:
The sentinel node occult lesion localization technique is a simple, reproducible and effective
alternative approach to occult lesions compared to other methods, such as mammotomy and the
hook-wire localization technique, for mapping suspect breast lesions and identifying lymph node
metastasis.
ROLL TECHNIQUE
Radioguided occult lesion localization (ROLL) has emerged as a novel
technique in surgery of non palpable breast lesions inspired by sentinel
node biopsy (SNB).
The ROLL technique utilizes the same intratumorally injected
radiofarmaceutical that is used for lymphatic mapping and sentinel node
biopsy (SNB). In the same surgical procedure, this tracer can be used to
localize the primary tumor guided by the hand-held gamma probe.
In ROLL technique, radioisotope injection adjacent to or into the lesion is
performed under ultrasound or stereotactic guidance preoperatively.
Since its first description in 1996 at the European Institute of Oncology in
Milan, this technique has allowed easier, more accurate and faster
removal of breast lesions than wire localization.
Routine ROLL involves the injection of 99mTc-labelled human serum
albumin into the suspicious lesion under ultrasonography or
mammography control within 24 h prior to surgery. Subsequently,
surgical excision is performed with the help of a hand-held gamma probe.
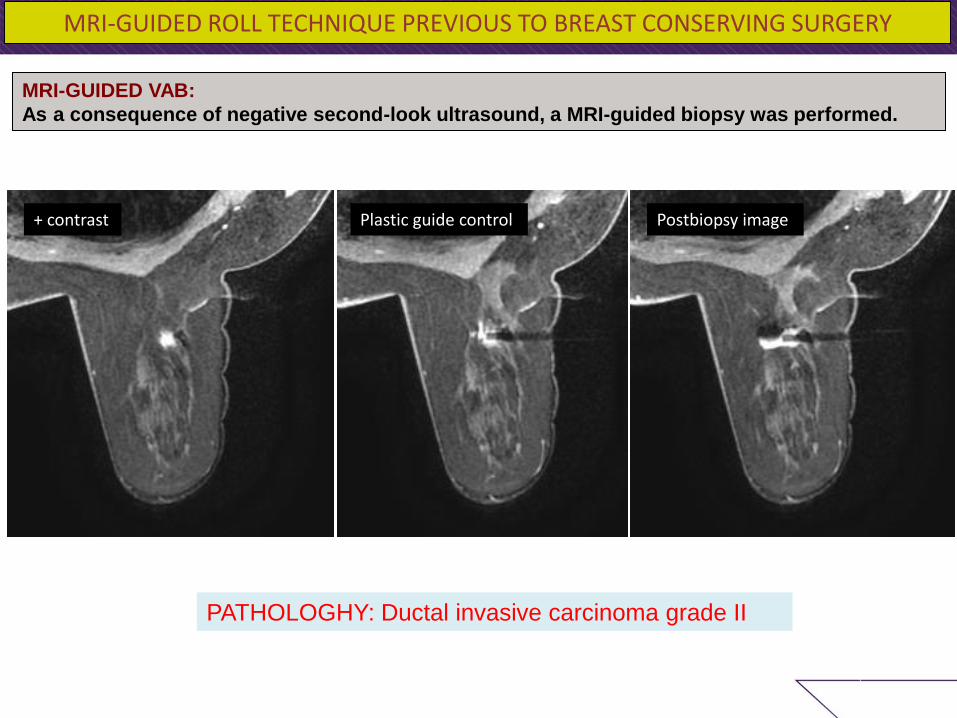
MRI-GUIDED VAB:
As a consequence of negative second-look ultrasound, a MRI-guided biopsy was performed.
PATHOLOGHY: Ductal invasive carcinoma grade II
+ contrast Plastic guide control Postbiopsy image
MRI-GUIDED ROLL TECHNIQUE PREVIOUS TO BREAST CONSERVING SURGERY
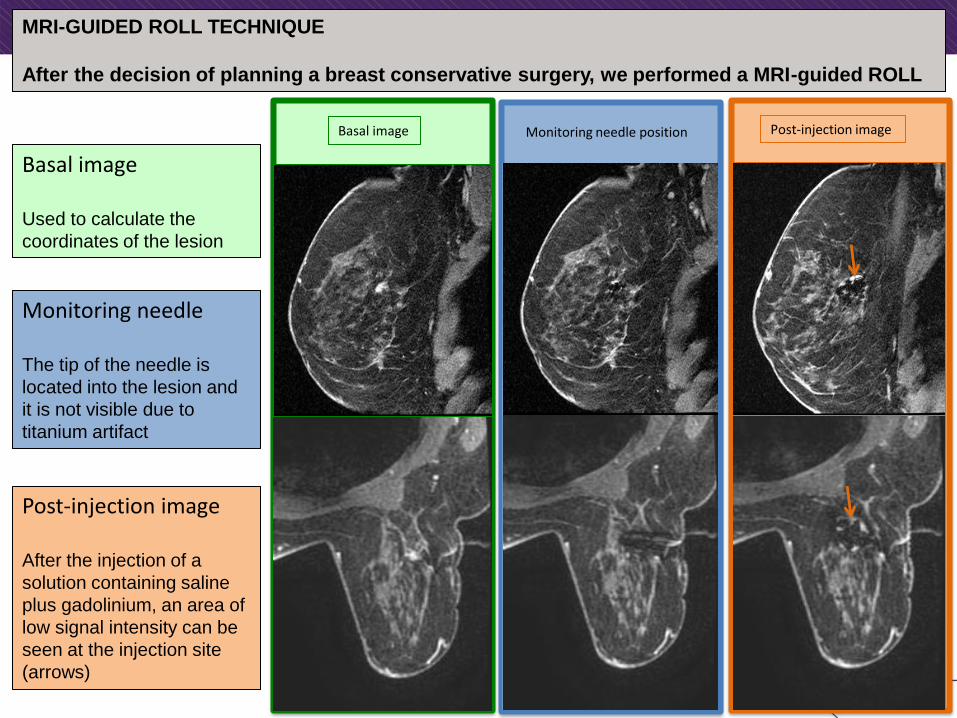
MRI-GUIDED ROLL TECHNIQUE
After the decision of planning a breast conservative surgery, we performed a MRI-guided ROLL
Basal image Monitoring needle position Post-injection image
Basal image Used to calculate the
coordinates of the lesion
Monitoring needle The tip of the needle is
located into the lesion and
it is not visible due to
titanium artifact
Post-injection image After the injection of a
solution containing saline
plus gadolinium, an area of
low signal intensity can be
seen at the injection site
(arrows)
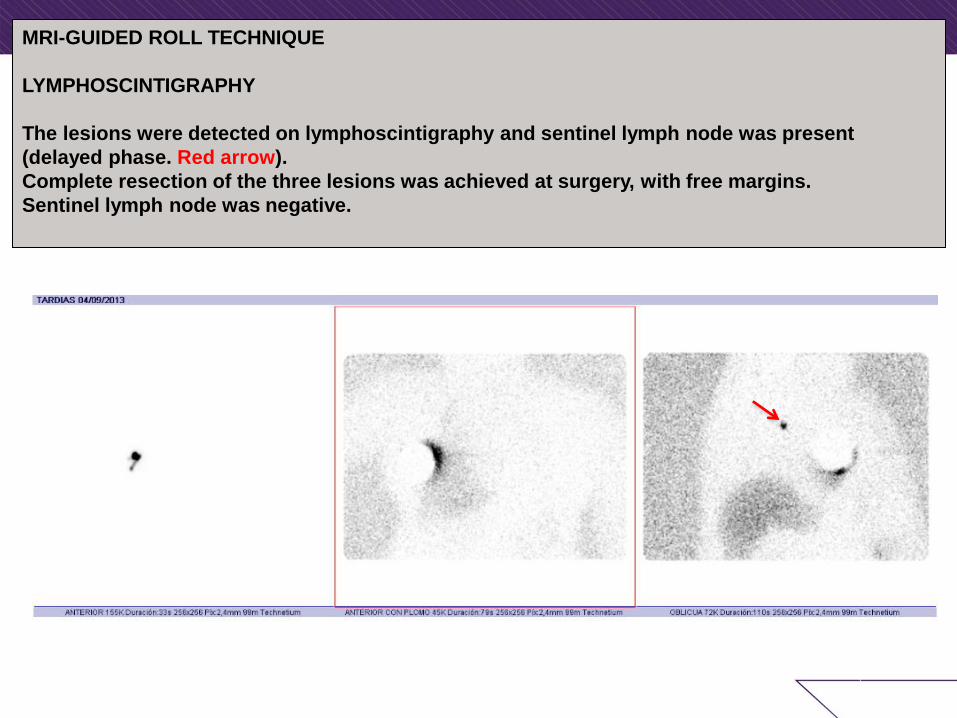
MRI-GUIDED ROLL TECHNIQUE
LYMPHOSCINTIGRAPHY
The lesions were detected on lymphoscintigraphy and sentinel lymph node was present
(delayed phase. Red arrow).
Complete resection of the three lesions was achieved at surgery, with free margins.
Sentinel lymph node was negative.
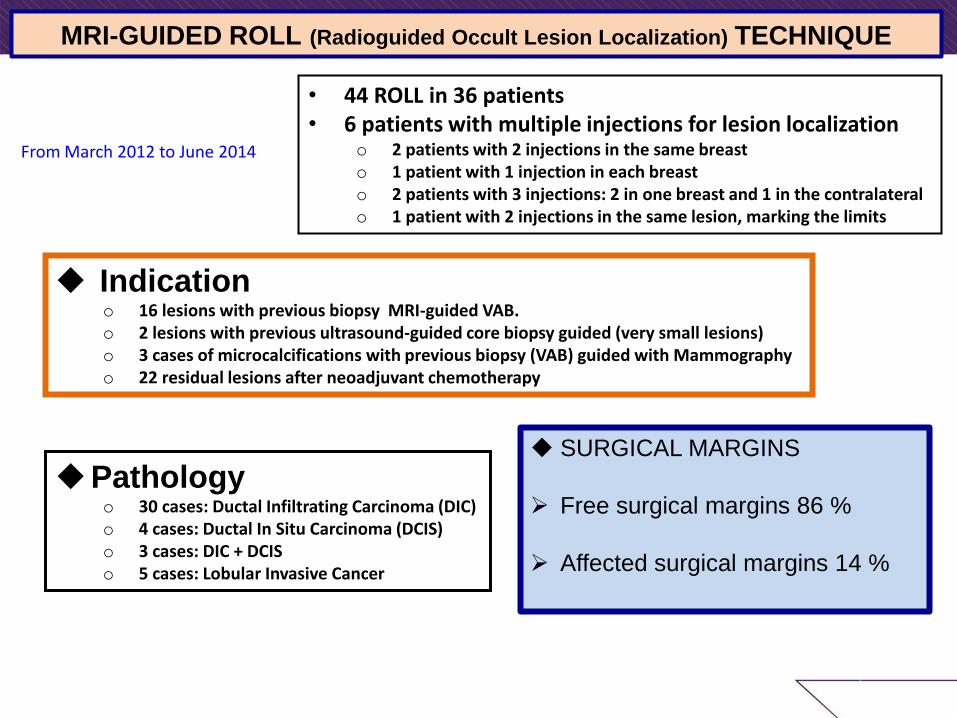
MRI-GUIDED ROLL (Radioguided Occult Lesion Localization) TECHNIQUE
• 44 ROLL in 36 patients • 6 patients with multiple injections for lesion localization
o 2 patients with 2 injections in the same breast o 1 patient with 1 injection in each breast o 2 patients with 3 injections: 2 in one breast and 1 in the contralateral o 1 patient with 2 injections in the same lesion, marking the limits
Indication o 16 lesions with previous biopsy MRI-guided VAB. o 2 lesions with previous ultrasound-guided core biopsy guided (very small lesions) o 3 cases of microcalcifications with previous biopsy (VAB) guided with Mammography o 22 residual lesions after neoadjuvant chemotherapy
Pathology o 30 cases: Ductal Infiltrating Carcinoma (DIC) o 4 cases: Ductal In Situ Carcinoma (DCIS) o 3 cases: DIC + DCIS o 5 cases: Lobular Invasive Cancer
From March 2012 to June 2014
SURGICAL MARGINS
Free surgical margins 86 %
Affected surgical margins 14 %
RM DE MAMA Y DIFUSIÓN
World J Surg Oncol. 2015 Feb 7;13:32. doi: 10.1186/s12957-014-0431-3.
Differential diagnosis of benign and malignant breast masses using diffusion-
weighted magnetic resonance imaging. Min Q1, Shao K2, Zhai L3, Liu W4, Zhu C5, Yuan L6, Yang J7.
RESULTS:
A total of 49 (49/52, 94.2%) lesions were detected using DW-MRI, including 20 benign
lesions (two lesions detected in the same patient) and 29 malignant lesions. Benign lesion
had a higher mean ADC value than their malignant counterparts, regardless of b value.
According to the receiver operating characteristic (ROC) curve, the smaller-range ROI was
more effective in differentiation between benign and malignant lesions. The area under the
ROC curve was the largest at a b value of 800 s/mm(2). With a threshold ADC value at
1.23 × 10(-3) mm(2)/s, DW-MRI achieved a sensitivity of 82.8%, specificity of 90.0%,
positive predictive value of 92.3%, and positive likelihood ratio of 8.3 for differentiating
benign and malignant lesions.
CONCLUSIONS:
DW-MRI is an accurate diagnostic tool for differentiation between benign and
malignant breast lesions, with an optimal b value of 800 s/mm(2). A smaller-range ROI
focusing on the highest signal has a better differential value.
RM DE MAMA Y ECOGRAFÍA SECOND-LOOK
DIAGNÓSTICOS Ultraschall Med. 2015 Apr;36(2):140-148. Epub 2015 Mar 6.
Role of Second-Look Ultrasound Examinations for MR-Detected Lesions in Patients
with Breast Cancer. Lee SH1, Kim SM2, Jang M2, Yun BL2, Kang E3, Kim SW3, Park SY4, Ahn HS5, Chang JH6, Yoo Y6, Song TK6, Moon WK1.
Results: According to the BI-RADS system, 67 lesions (50.8 %) were classified as category 0, 33 lesions (25.0 %) as category 3, and
32 lesions (24.2 %) as category 4. Of the 67 indeterminate lesions on MR imaging, 34 (50.7 %) were demonstrated on second-look US. 11 of these 34 lesions showed suspicious sonographic features, including 1 lesion that showed malignancy (9.1 %, 1/11). Most of the suspicious lesions on MR imaging (26 of 32 BI-RADS category 4 lesions, 81.3 %) were demonstrated on second-look US, and 17 were malignant (65.4 %, 17/26). Of the 6 BI-RADS category 4 lesions without sonographic correlation, 1 was malignant (16.7 %, 1/6)
Conclusion: Second-look US examination was useful for evaluating MR-detected lesions in patients with breast cancer.
Ultrasonography. 2015 Apr;34(2):125-32. doi: 10.14366/usg.14046. Epub 2014 Dec 18.
Second-look ultrasonography for MRI-detected suspicious breast lesions in patients
with breast cancer. Hong MJ1, Cha JH1, Kim HH1, Shin HJ1, Chae EY1, Shin JE2, Choi WJ1.
CONCLUSION: We have concluded that second-look US is a useful diagnostic tool for lesions incidentally detected on breast MRI, as in
this study, it could identify 86.8% of the MRI-detected breast lesions.
¡¡¡LA ECOGRAFÍA ES LA MEJOR AMIGA DE LA RESONANCIA DE MAMA!!!
RM DE MAMA Y CRIBADO EN PACIENTES DE ALTO RIESGO
J Clin Oncol. 2015 Apr 1;33(10):1128-35. doi: 10.1200/JCO.2014.56.8626. Epub 2015 Feb 23.
Triple-modality screening trial for familial breast cancer underlines the importance of
magnetic resonance imaging and questions the role of mammography and ultrasound
regardless of patient mutation status, age, and breast density. Riedl CC1, Luft N2, Bernhart C2, Weber M2, Bernathova M2, Tea MK2, Rudas M2, Singer CF2, Helbich TH2.
RESULTS:
There were 559 women with 1,365 complete imaging rounds included in this study. The sensitivity of
MRI (90.0%) was significantly higher (P < .001) than that of mammography (37.5%) and ultrasound
(37.5%). Of 40 cancers, 18 (45.0%) were detected by MRI alone. Two cancers were found by
mammography alone (a ductal carcinoma in situ [DCIS] with microinvasion and a DCIS with < 10-
mm invasive areas). This did not lead to a significant increase of sensitivity compared with using MRI
alone (P = .15). No cancers were detected by ultrasound alone. Similarly, of 14 DCISs, all were
detected by MRI, whereas mammography and ultrasound each detected five DCISs (35.7%). Age,
mutation status, and breast density had no influence on the sensitivity of MRI and did not affect the
superiority of MRI over mammography and ultrasound.
CONCLUSION:
MRI allows early detection of familial breast cancer regardless of patient age, breast density, or
risk status. The added value of mammography is limited, and there is no added value of
ultrasound in women undergoing MRI for screening.
RM DE MAMA Y CRIBADO EN PACIENTES DE ALTO RIESGO
J Clin Oncol. 2015 Feb 1;33(4):349-56. doi: 10.1200/JCO.2014.56.6232. Epub 2014 Dec 22.
Magnetic resonance imaging improves breast screening sensitivity in
BRCA mutation carriers age ≥ 50 years: evidence from an individual
patient data meta-analysis. Phi XA1, Houssami N1, Obdeijn IM1, Warner E1, Sardanelli F1, Leach MO1, Riedl CC1, Trop I1, Tilanus-Linthorst MM1, Mandel R1, Santoro F1, Kwan-Lim G1,
Helbich TH1, de Koning HJ1, Van den Heuvel ER1, de Bock GH2.
RESULTS:
Pooled analysis showed that in women age ≥ 50 years, screening sensitivity was not different from
that in women age < 50 years, whereas screening specificity was. In women age ≥ 50 years,
combining MRI and mammography significantly increased screening sensitivity compared with
mammography alone (94.1%; 95% CI, 77.7% to 98.7% v 38.1%; 95% CI, 22.4% to 56.7%; P <
.001). The combination was not significantly more sensitive than MRI alone (94.1%; 95% CI,
77.7% to 98.7% v 84.4%; 95% CI, 61.8% to 94.8%; P = .28). Combining MRI and mammography
in women age ≥ 50 years resulted in sensitivity similar to that in women age < 50 years (94.1%;
95% CI, 77.7% to 98.7% v 93.2%; 95% CI, 79.3% to 98%; P = .79).
CONCLUSION:
Addition of MRI to mammography for screening BRCA1/2 mutation carriers age ≥ 50 years
improves screening sensitivity by a magnitude similar to that observed in younger women. Limiting
screening MRI in BRCA1/2 carriers age ≥ 50 years should be reconsidered.
RM DE MAMA Y CRIBADO EN PACIENTES DE ALTO RIESGO
Breast Cancer Res Treat. 2014 Oct;147(3):685-7. doi: 10.1007/s10549-014-3097-1. Epub 2014 Sep 2.
MRI screening of women with hereditary predisposition to breast
cancer: diagnostic performance and survival analysis. Santoro F1, Podo F, Sardanelli F.
DISCUSSION AND CONCLUSIONS: The capability of MRI to detect invasive breast cancers at early stages could at least
partly explain the significantly higher 10-year survival estimated by Gareth et al for
asymptomatic highrisk women screened using MRI in the period 1997-2013 (95 %)
compared with unscreened high-risk women diagnosed for breast cancer after 1990 and
identified as BRCA1/BRCA2 mutation carriers in the years following diagnosis (74
%). It appears however worth noting that the evolution of therapeutic protocols applied
to high-risk patients after the discovery of BRCA mutations in 1995-1997 could also
have contributed to the observed difference in the survival of these two groups. On the
other hand, we agree with Gareth et al that larger datasets are needed to evaluate to
which extent improvements in the cancer detection impact on disease-free and overall
survival of MRI-screened compared with mammography-alone-screened high-risk
women
RM DE MAMA Y QUIMIOTERAPIA
Eur Radiol. 2015 Apr;25(4):1097-106. doi: 10.1007/s00330-014-3502-5. Epub 2014 Nov 26.
Prognostic value of DCE-MRI in breast cancer patients undergoing
neoadjuvant chemotherapy: a comparison with traditional survival
indicators. Pickles MD1, Lowry M, Manton DJ, Turnbull LW.
CONCLUSIONS: Multivariate survival analysis has demonstrated that DCE-MRI parameters obtained prior
to NAC and/or post 2nd cycle can provide independent prognostic information that can
complement traditional prognostic indicators available prior to treatment.
KEY POINTS: • MR-derived DCE-MRI parameters obtained prior to treatment have prognostic value. •
Early treatment-induced reductions in DCE-MRI parameters represents a positive
prognostic indicator. • DCE-MRI parameters provide independent prognostic information
that can complement traditional prognostic indicators.
Background
• A pathologic confirmed complete response
(pCR) after neoadjuvant chemotherapy (NAC)
is consistently asssociated with disease-free
and overall survival benefit1.
• pCR occurs in a subgroup of patients and
several markers have been used to predict
outcome and to select therapy. Estrogen
receptor (ER), progesterone receptor (PR) and
human epidermal growth factor receptor 2
(HER2/neu) are the most frequently used
markers2.
• MRI has proved the most accurate imaging
method to address treatment response to
NAC in breast cancer patients3.
• However, its ability to predict pCR in
histologically different tumors remains
unclear3,4.
• We tried to investigate the usefulness of MRI
in evaluation of pCR in different breast cancer
subtypes after treatment with NAC
• Serial MRI studies were acquired before,
during and after NAC in 75 evaluable patients.
• MRI interpretation included lesion size,
morphology and dynamic enhanced
evaluation imaging with initial and late
enhancement.
• On the basis of the final MRI, response was
determined to be a clinically complete
response (CCR) when no residual tumor and
no late enhancement were found.
• By using inmunohistochemistry and
fluorescence in situ hybridization (FISH) for
HER2/neu amplification, tumors were divided
into three subtypes: triple negative, HER2
positive, and ER positive/HER2 negative.
• Every patient received chemotherapy with
taxanes and anthracyclines and HER2 positive
tumors were treated with trastuzumab.
• All patients received surgery.
• pCR was defined as no residual invasive
tumor in the surgical specimen. Ductal
carcinoma in situ residual disease was
considered pCR.
Methods
Results
Conclusion
Absence of both residual tumor and late
enhancement in MRI predict pCR with high
accuracy in triple negative, HER2 positive
and ER positive/HER2 negative breast
cancer after NAC.
Lucia Gonzalez-Cortijo, Javier Hornedo, Ricardo Sainz de la Cuesta, Gines Hernandez-Cortes, Ramon Perez-Carrion,
Federico Gonzalez, Agustin Acevedo, Elia del Cerro, Susana Linares,
Antonio Maldonado, Antonio Cabrera, Felipe Counago, Ana Diaz-Gavela, Cristina Rodriguez-
Marquez, Mercedes Espada, Alexandra Henriquez, Raquel Murillo,
Jose Luis Martin del Yerro, Ignacio Sanz, Manuel Recio, Vicente Martinez de Vega.
Quiron Madrid University Hospital. Madrid, Spain.
References
1. Rastogi P, Anderson SJ, Bear HD, et al:
Preoperative chemotherapy: Updates of
National Surgical Adjuvant Breast and
Bowel Project Proto- cols B-18 and B-27. J
Clin Oncol 26:778-785, 2008
2. Straver ME, Rutgers EJ, Rodenhuis S, et al:
The relevance of breast cancer subtypes in
the outcome of neoadjuvant chemotherapy.
Ann Surg Oncol 17:2411-2418, 2010
3. Chen JH, Feig B, Agrawal G, et al: MRI
evaluation of pathologically complete
response and residual tumors in breast
cancer after neoadjuvant chemotherapy.
Cancer 112:17-26, 2008
4. Loo CE, Straver ME, Rodenhuis S, et al:
Magnetic resonance imaging response
monitoring of breast cancer during
neoadjuvant chemotherapy: relevance of
breast cancer subtype. J Clin Oncol 29:
660-666, 2011
Abstr. 1111
• 22 of 75 patients (29%) achieved a
CCR on the final MRI.
• Of 22 patients with CCR all 22 (100%)
were confirmed pathologically. 19
were pathologic complete responses
and 3 showed in situ microscopic
residual disease.
• 12 (55%) were HER2 positive tumors,
• 4 (18%) were triple negative tumors
• 6 (27%) were ER positive/HER2
negative tumors.
• The negative predictive value of MRI
for predicting pCR after NAC was
100%.
RESULTS
•Of 22 patients with pCR all 22 (100%) were confirmed
pathologically. 19 were pathologic complete responses and
3 showed in situ microscopic residual disease.
•12 (55%) were HER2 positive tumors,
•4 (18%) were triple negative tumors
•6 (27%) were ER positive/HER2 negative tumors.
•The negative predictive value of MRI for predicting pCR
after NAC was 100%.
CONCLUSION
Absence of both residual tumor and late
enhancement in MRI predict pCR with
high accuracy in triple negative, HER2
positive and ER positive/HER2 negative
breast cancer after NAC.
RM DE MAMA Y PAPILOMAS
Clin Imaging. 2015 Feb 7. pii: S0899-7071(15)00042-X. doi: 10.1016/j.clinimag.2015.01.017. [Epub ahead of print]
Outcomes of benign breast papillomas diagnosed at image-guided vacuum-assisted core
needle biopsy. Hawley JR1, Lawther H2, Erdal BS3, Yildiz VO4, Carkaci S5.
CONCLUSION:
Benign papillomas diagnosed with VACNB demonstrated a 3% upgrade rate to malignancy, which is similar to the
2.9% upgrade rate calculated by compiling applicable published literature. Conservative management with imaging
follow-up as opposed to surgical excision may be appropriate in cases where an initial diagnosis of benign papilloma is
made with VACNB. Benign papillomas associated with calcifications on imaging should be considered for
surgical excision given their increased association with malignancy.
Biomed Res Int. 2015;2015:806368. doi: 10.1155/2015/806368. Epub 2015 Jan 22.
Breast MRI in patients with unilateral bloody and serous-bloody nipple discharge: a
comparison with galactography. Manganaro L1, D'Ambrosio I1, Gigli S1, Di Pastena F1, Giraldi G2, Tardioli S1, Framarino M3, Porfiri LM1, Ballesio L1.
RESULTS:
After surgery and follow-up, 8 patients had no disease (15%), 23 papilloma (43%), 11 papillomatosis (21%), 5 ductal
cancer in situ (10%), and 6 papillary carcinoma (11%) diagnoses. Both techniques presented 100% specificity; MRI
sensitivity was 98% versus 49% of galactography. Considering MRI, we found a statistical association between mass
enhancement and papilloma (P < 0.001; AUC 0.957; CI 0.888-1.025), ductal enhancement and papillomatosis (P <
0.001; AUC 0.790; CI 0.623-0.958), segmental enhancement and ductal cancer in situ (P = 0.007; AUC 0.750; CI
0.429-1.071), and linear enhancement and papillary cancer (P = 0.011).
CONCLUSIONS:
MRI is a valid tool to detect ductal pathologies in patients with suspicious bloody or serous-bloody discharge showing
higher sensitivity and specificity compared to galactography.
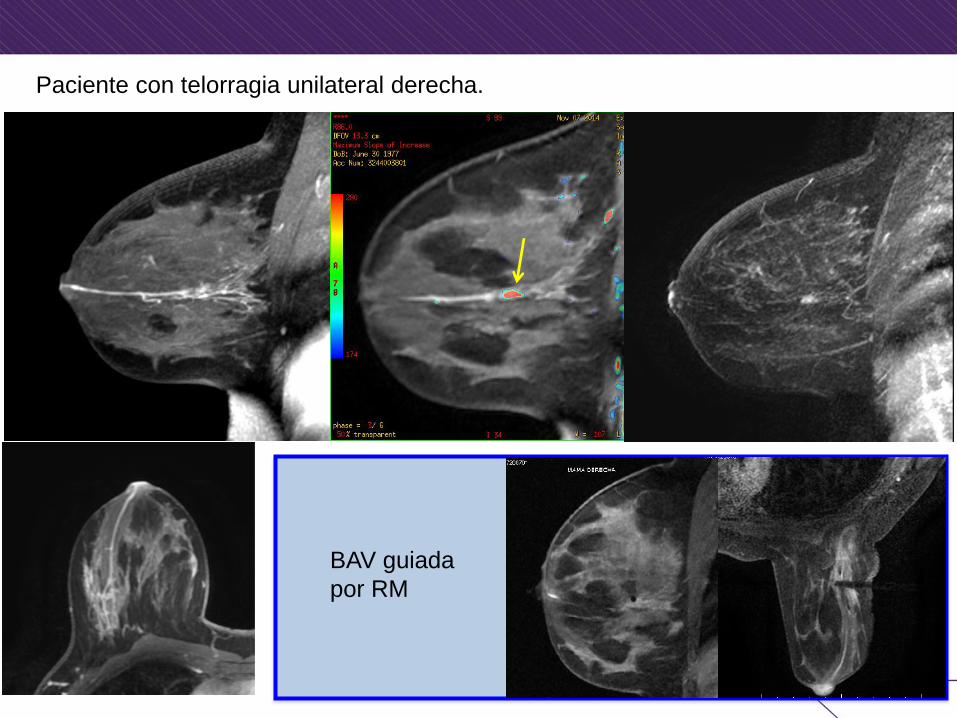
Paciente con telorragia unilateral derecha.
BAV guiada
por RM

Control 6 meses tras biopsia excisional. Desaparición de la telorragia
Desaparición del papiloma y del ducto dilatado con sangre en su interior
RM DE MAMA Y CARACTERIZACIÓN DE LESIONES Radiology. 2015 Feb;274(2):343-51. doi: 10.1148/radiol.14140645. Epub 2014 Sep 29.
Assessment of BI-RADS category 4 lesions detected with screening mammography and
screening US: utility of MR imaging. Strobel K1, Schrading S, Hansen NL, Barabasch A, Kuhl CK.
RESULTS:
Of the 353 study findings, 66 (18.7%) were finally shown to be true-positive (23 cases of ductal
carcinoma in situ [DCIS], 43 invasive cancers) and 287 (81.3%) were false-positive. Assessment of MR
imaging findings led to a correct diagnosis of no breast cancer in 264 of the 287 false-positive findings
(92%) and helped confirm the presence of breast cancer in 63 of 66 malignancies. The false-negative rate
for pure clustered microcalcifications was 12% (three of 25 cases) because of three nonenhancing low-
grade DCIS cases; in turn, MR imaging depicted additional invasive cancers in three women with false-
positive findings from mammography and US. For mammographic findings other than pure clustered
microcalcifications, MR imaging increased the positive predictive value (PPV) from 17.5% (21 of 120
cases; 95% confidence interval [CI]: 10.7%, 24.3%) to 78% (21 of 27 cases; 95% CI: 62.1%, 93.5%),
with a false-negative rate of 0%. For all US findings, MR imaging increased the PPV from 12.9% (20 of
155 cases; 95% CI: 7.6%, 18.2%) to 69% (20 of 29 cases; 95% CI: 52.2%, 85.8%), again with a false-
negative rate of 0%. MR imaging resulted in false-positive findings that led to MR imaging-guided
biopsy in five of the 340 patients (1.5%).
CONCLUSION:
MR imaging is useful for the noninvasive work-up of lesions classified as BI-RADS category 4 at
mammography or US and can help avoid 92% of unnecessary biopsies. The false-negative rate was
0% for all US findings and for all mammographic findings except pure clustered
microcalcifications. Additional invasive cancers were identified in three women with false-positive
findings from mammography and US.
RM DE MAMA Y CARACTERIZACIÓN DE LESIONES
Breast J. 2014 Nov-Dec;20(6):622-31. doi: 10.1111/tbj.12334. Epub 2014 Sep 8.
Magnetic resonance imaging of the breast as a problem-solving method: to be or not to be? Oztekin PS1, Kosar PN.
In cases with inconclusive findings on conventional imaging studies or in patients with clinical/radiological suspicion of malignancy, MRI should be more effectively used as a problem-solving approach owing to its high sensitivity and NPV in this condition. Use of MRI as a problem-solving method in such cases may decrease rather than increase unnecessary biopsy procedures and patient anxiety.
Acta Radiol. 2015 May 20. pii: 0284185115585036. [Epub ahead of print]
MRI and comparison mammography: a worthy diagnostic alliance for breast
microcalcifications? Brnic D1, Brnic D2, Simundic I3, Vanjaka Rogosic L4, Tadic T3.
RESULTS:
Of the 55 microcalcification cases, 35 showed progression and 20 were stable between interval screenings. The
negative predictive value (NPV) of comparison mammography was 100%, whereas the NPV of MRI was 92%.
However, the specificity of combination of findings was 97%, significantly higher than the 42% specificity of
comparison mammography (P < 0.001). Additionally, the positive predictive value of combination of findings was 93%
versus 44% of comparison mammography (P = 0.001).
CONCLUSION:
A biopsy is recommended when MRI positive lesion corresponding the area of new or increasing
mammographic microcalcifications is detected. Patients with stable microcalcifications can continue
follow-up mammography, regardless of MRI result.
RM Y TAMAÑO TUMORAL
Eur J Radiol. 2015 Apr;84(4):603-10. doi: 10.1016/j.ejrad.2014.12.016. Epub 2015 Jan 7.
Comparison of 3.0 T magnetic resonance imaging and X-ray
mammography in the measurement of ductal carcinoma in situ: a
comparison with histopathology. Pickles MD1, Gibbs P2, Hubbard A3, Rahman A3, Wieczorek J3, Turnbull LW2.
RESULTS:
Data from 39 patients with a median age of 55 years (range 38-78 years) underwent analysis.
Mastectomy was undertaken in 21 cases, while breast conserving surgery was performed in 18
subjects. Histopathological analysis revealed one low grade, nine intermediate grade, and 21 high
grade lesions. The mean±standard deviation LD measurements for histopathology, X-ray
mammography and MRI were 50.6±34.2 mm, 30.7±23.1 mm and 49.6±26.8 mm respectively.
Bland-Altman agreement plot analysis for the whole cohort revealed not only a smaller
logarithmic mean difference between MRI and histopathology (0.086), but also narrower 95% LoA
(-0.941 to 1.113) compared with X-ray mammography and histopathology (mean difference -
0.658, 95% LoA -3.503 to 2.187). When the level of agreement was assessed between clinically
relevant subgroups additional significant differences were noted based on grade, hormonal
receptor status, invasion, necrosis, mircocalcifications and growth pattern.
CONCLUSION:
MRI provides a more accurate estimation of DCIS size than X-ray mammography. MRI's
superior ability was not only noted in general, but also for clinical relevant subdivisions such as
grade and the presence or absence of necrosis.
MAMOGRAFÍA
Cancer. 2015 Apr 14. doi: 10.1002/cncr.29371. [Epub ahead of print]
Effect of treatment and mammography detection on breast cancer survival over time:
1990-2007. Kaplan HG1, Malmgren JA2,3, Atwood MK1, Calip GS4.
BACKGROUND:
The extent to which improvements over time in breast cancer survival are related to earlier detection by mammography or to more
effective treatments is not known.
METHODS:
At a comprehensive cancer care center, the authors conducted a retrospective cohort study of women ages 50 to 69 years who were
diagnosed with invasive breast cancer (stages I through III) and were followed over 3 periods (1990-1994, 1995-1999, and 2000-2007).
Data were abstracted from patient charts and included detection method, diagnosis, treatment, and follow-up for vital status in the
institutional breast cancer registry (n = 2998). The method of detection was categorized as patient or physician detected or
mammography detected. Cox proportional hazards models were used to estimate adjusted hazard ratios (HRs) and 95% confidence
intervals (CIs) for 5-year disease-specific survival in relation to detection method and treatment factors, and differences in survival were
analyzed using the Kaplan-Meier method.
RESULTS:
Fifty-eight percent of breast cancers were mammography detected, and 42% were patient or physician detected; 56% of tumors were
stage I, 31% were stage II, and 13% were stage III. The average length of follow-up was 10.71 years. The combined 5-year disease-
specific survival rate was 89% from 1990 to 1994, 94% from 1995 to 1999, and 96% from 2000 to 2007 (P < .001). In an adjusted
model, mammography detection (HR, 0.43; 95% CI, 0.27-0.70), hormone therapy (HR, 0.47; 95% CI, 0.30-0.75), and taxane-containing
chemotherapy (HR, 0.61; 95% CI, 0.37-0.99) were significantly associated with a decreased risk of disease-specific mortality.
CONCLUSIONS:
Better breast cancer survival over time was related to mammography detection, hormone therapy, and taxane-
containing chemotherapy. Treatment improvements alone are not sufficient to explain the observed survival
improvements over time. Cancer 2015. © 2015 American Cancer Society.
Aproximadamente 1200 artículos publicados (Junio 2014- Junio 2015)
MAMOGRAFÍA (TOMOSÍNTESIS)
Breast Cancer Screening Using Tomosynthesis in Combination With
Digital Mammography. JAMA. 2014;311(24):2499-2507. doi:10.1001/jama.2014.6095. Friedewald S M, Rafferty E A, Rose S L, , Durand M A, Plecha D M, Greenberg J S, Hayes M K, Copit D S,
Carlson K L, Cink T M, Barke L D, Greer L N, Miller D P, Conant E F.
* Key Point: In this largest screening study involving over 450,000 examinations, the
authors conclude that the addition of 3D mammography to 2D mammography
demonstrated an increase in cancer detection rate and a decrease in the recall rate. The
authors also conclude that the PPV3 improved by 21% after the introduction of tomosynthesis.
Breast screening using 2D-mammography or integrating digital breast
tomosynthesis (3D-mammography) for single-reading or
doublereading- Evidence to guide future screening strategies. Eur J Cancer.2014 Jul;50(10):1799-807.
Houssami N, Macaskill P, Bernardi D, Caumo F, Pellegrini M, Brunelli S, Tuttobene P, Bricolo P,
Fantò C, Valentini M, Ciatto S.
* Key Point: Combined 2D/3D-mammography was found to offer significantly higher
cancer detection than 2D mammography using either single or double reading.
MAMOGRAFÍA (TOMOSÍNTESIS)
Comparison with Synthetic 2D Mammography Reconstructed from
Digital Breast Tomosynthesis and Digital 2D Mammography for the
Detection of T1 Breast Cancer. Radiological Society of North America 2014 Scientific Assembly and Annual Meeting, November
30 - December 5, 2014, Chicago IL.
Choi J, Han B, Ko E, Ko E, Hahn S.
* Key Point: The authors conclude that the diagnostic performance was similar for
synthetic 2D mammography compared to digital 2D mammography. The authors also
suggest that the use of synthetic mammogram may reduce the radiation dose in patients,
since the resultsindicate that 2D mammography may not be necessary during the
tomosynthesis-based screening.
The STORM II (Screening with Tomosynthesis or Mammography II)
Trial: Interim Comparison of Screen-reading Strategies in Population
Breast Screening. Radiological Society of North America 2014 Scientific Assembly and Annual Meeting, November
30 - December 5, 2014, Chicago IL.Bernardi D, Pellegrini M, Valentini M, Fanto C, Houssami N.
* Key Point: The authors conclude integrated synthetic 2D with 3D mammography had
a comparable cancer detection compared to integrated standard 2D and 3D, thus reducing
the radiation dose in patients undergoing tomosynthesis-based screening.
MAMOGRAFÍA (TOMOSÍNTESIS)
Two-view digital breast tomosynthesis screening with synthetically
reconstructed projection images: comparison with digital breast
tomosynthesis with full-field digital mammographic images. Radiology. 2014 Jun;271(3):655-63.
Skaane P, Bandos AI, Eben EB, Jebsen IN, Krager M, Haakenaasen U, Ekseth U, Izadi M,
Hofvind S, Gullien R.
* Key Point: The authors conclude that the use of generated 2D images constituted an
average dose reduction of 45% while not resulting in any clinically meaningful
differences in diagnostic accuracy
MAMOGRAFÍA (TOMOSÍNTESIS)
Utilizing digital breast tomosynthesis to improve accuracy of
preoperative needle localization for surgical excisional biopsy. Del Med J. 2015 Apr;87(4):117-20. Hasan R, Gavenonis SC, Shin MC.
Abstract We describe a case of an 88-year-old female who presented for needle localization to undergo excisional
biopsy of a subtle asymmetry in the left breast, with successful localization achieved using digital breast
tomosynthesis. Initial attempts at localization under 2D mammography were inaccurate. Subsequent digital
breast tomosynthesis application for triangulation resulted in better visualization of the target, and successful
localization. Specimen radiography confirmed the lesion was accurately targeted and pathology revealed
ductal carcinoma in situ. Needle localization guided by mammography and inherent limitations of 2D
mammography are discussed, along with a literature review of tomosynthesis guided needle localization.
Digital breast tomosynthesis-guided vacuum-assisted breast biopsy: initial experiences and comparison with prone stereotactic vacuum-assisted biopsy. Radiology. 2015 Mar;274(3):654-62. doi: 10.1148/radiol.14141397. Epub 2014 Nov 11. Schrading S1, Distelmaier M, Dirrichs T, Detering S, Brolund L, Strobel K, Kuhl CK.
RESULTS: Technical success was achieved in 51 of 51 lesions (100%) with DBT VAB versus 154 of 165 lesions (93%) with PS VAB. In one of 11 lesions in which PS VAB
failed, DBT VAB was performed successfully. Mean time to complete VAB was 13 minutes ± 3.7 for DBT VAB versus 29 minutes ± 10.1 for PS VAB (P < .0001).
Reidentifying and targeting lesions during PS VAB took longer than it did during DBT VAB (P < .0001). Tissue sampling took about the same time for PS VAB and
DBT VAB (P = .067). Significantly more "low-contrast" (ie, uncalcified) target lesions were biopsied with DBT VAB (13 of 51 lesions) versus PS VAB (nine of 165
lesions) (P < .0002). No major complications were observed with either system. One patient who underwent DBT VAB in the sitting position and one patient who
underwent PS VAB developed self-limiting vasovagal reactions.
CONCLUSION: Clinical performance of DBT VAB was significantly superior to PS VAB. Because DBT VAB allows use of the full detector size for imaging and provides immediate
lesion depth information without requiring triangulation, it facilitates target lesion reidentification and sampling of even low-contrast targets, such as uncalcified masses.
ECOGRAFÍA
Eur J Radiol. 2015 Jul;84(7):1232-5. doi: 10.1016/j.ejrad.2015.04.007. Epub 2015 Apr 20.
The image quality and lesion characterization of breast using automated
whole-breast ultrasound: A comparison with handheld ultrasound.
OBJECTIVE: To prospectively evaluate the image quality of automated whole breast ultrasonography (AWUS) in the characterization of
breast lesions compared with handheld breast ultrasonography (HHUS).
MATERIALS AND METHODS: This prospective study included a total of 411 lesions in 209 women. All patients underwent both HHUS and AWUS prior to biopsy. An evaluation of identical image pairs
of 411 lesions obtained from both modalities was performed, and the image quality of AWUS was compared with that of HHUS as a reference standard. The overall image
quality was evaluated for lesion coverage, lesion conspicuity, and artifact effect using a graded score. Additionally, the factors that correlated with differences in image
quality between the two modalities were analyzed.
RESULTS: In 97.1%, the image quality of AWUS was identical or superior to that of HHUS, whereas AWUS was inferior in 2.9%. In only
0.5%, the poor quality of AWUS images caused by incomplete lesion coverage and shadowing due to a contact artifact inhibited
precise interpretations. The two main causes resulting in degraded AWUS image quality were blurring of the margin (83.3%) and
acoustic shadowing by Cooper's ligament or improper compression pressure of the transducer (66.7%). Among various factors,
peripheral location from the nipple (p=0.01), lesion size (p=0.02), shape descriptor (p=0.02), and final American College of
Radiology Breast Imaging Reporting and Data System (BI-RADS) category (p=0.001) were correlated with differences in image
quality between AWUS and HHUS.
CONCLUSION: Although the image quality of AWUS was comparable to that of HHUS for lesion interpretation, HHUS was clearly
superior to AWUS for analyzing lesions with a peripheral location, an irregular shape, a non-circumscribed margin and BI-
RADS category 4 or 5.
Aproximadamente 800 artículos publicados (Junio 2014- Junio 2015)
ECOGRAFÍA
Asian Pac J Cancer Prev. 2014;15(21):9101-5.
Comparison of automated breast volume scanning and hand-
held ultrasound in the detection of breast cancer: an analysis of
5,566 patient evaluations. Choi WJ1, Cha JH, Kim HH, Shin HJ, Kim H, Chae EY, Hong MJ.
BACKGROUND:
The purpose of this study was to compare the accuracy and effectiveness of automated breast volume scanning
(ABVS) and hand-held ultrasound (HHUS) in the detection of breast cancer in a large population group with a long-
term follow-up, and to investigate whether different ultrasound systems may influence the estimation of cancer
detection.
MATERIALS AND METHODS: Institutional review board approval was obtained for this retrospective study, and informed consent was waived. From September 2010 to August 2011, a total of
1,866 ABVS and 3,700 HHUS participants, who underwent these procedures at our institute, were included in this study. Cancers occurring during the study and
subsequent follow-up were evaluated. The reference standard was a combination of histology and follow-up imaging (≥12 months). The recall rate, cancer detection
yield, diagnostic accuracy, sensitivity, specificity, and positive (PPV) and negative (NPV) predictive values were calculated with exact 95% confidence intervals.
RESULTS: The recall rate was 2.57 per 1,000 (48/1,866) for ABVS and 3.57 per 1,000 (132/3,700) for HHUS, with ? significant
difference (p=0.048). The cancer detection yield was 3.8 per 1,000 for ABVS and 2.7 per 1,000 for HHUS. The
diagnostic accuracy was 97.7% for ABVS and 96.5% for HHUS with statistical significance (p=0.018). The
specificity of ABVS and HHUS were 97.8%, 96.7%, respectively (p=0.022).
CONCLUSIONS: ABVS shows a comparable diagnostic performance to HHUS. ABVS is an effective supplemental tool for
mammography in breast cancer detection in a large population.
ECOGRAFÍA
Eur Radiol. 2015 Mar 5. [Epub ahead of print]
The Z0011 Trial: Is this the end of axillary ultrasound in the pre-
operative assessment of breast cancer patients? Farrell TP1, Adams NC, Stenson M, Carroll PA, Griffin M, Connolly EM, O'Keeffe SA.
OBJECTIVES:
The Z0011 trial questioned the role of axillary ultrasound (AxUS) in preoperative staging of breast cancer in patients
with ≤2 positive sentinel lymph nodes (SLN). The purpose of this study was to correlate the number of abnormal nodes
on AxUS with final nodal burden and determine the utility of AxUS with sampling (AxUS + S) in preoperative staging.
METHODS: Six hundred and seventy-nine patients underwent pre-operative AxUS. Suspicious nodes were sampled. Negative axillae proceeded to SLN biopsy. The number of
abnormal nodes identified on ultrasound and final histology as well as sensitivity and specificity for AxUS + S were calculated. Subgroup analysis was performed on
Z0011 eligible patients.
RESULTS: Two hundred and ninety-six patients had positive axillary nodes on final histology with 169 detected by AxUS + S (sensitivity 86.2 %, specificity 100 %, PPV 100 %,
NPV 71.9 %). Patients with nodal metastases identified by AxUS had a mean burden of 7.3 nodes on histology (1 node on AxUS = 5.2 nodes on histology, 2 nodes on
AxUS = 7.5 nodes, >2 nodes = 10.1 nodes). Patients diagnosed on SLNB had a mean burden of 2.2 nodes.
CONCLUSION:
A single nodal metastasis detected on AxUS + S correlated with a mean of 5.2 nodes on final histology highlighting that
AxUS remains essential in guiding appropriate management of the axilla in breast cancer.
KEY POINTS: • Axillary ultrasound +/- sampling is an essential technique in preoperative axillary staging. • Axillary ultrasound
findings correlate with final histological axillary node disease burden. • Axillary ultrasound can help triage
patients who require axillary lymph node dissection. • The role of axillary ultrasound in breast cancer staging
continues to evolve.
ECOGRAFÍA
Breast Cancer Res Treat. 2015 Jun;151(2):347-55. doi: 10.1007/s10549-015-3388-1. Epub 2015 Apr 23.
The clinical utility of assessment of the axilla in women with
suspicious screen detected breast lesions in the post Z0011 era. Farshid G1, Kollias J, Grantley Gill P.
Abstract
Axillary ultrasound (AUS) and biopsy are now part of the preoperative assessment of breast cancer based on the
assumption that any nodal disease is an indication for axillary clearance (AC). The Z0011 trial erodes this assumption.
We applied Z0011 eligibility criteria to patients with screen detected cancers and positive axillary assessment to
determine the relevance of AUS to contemporary practice. Women screened between 1/1/2012 and 30/6/2013 and
assessed for lesions with highly suspicious imaging features are included. We analysed demographic and assessment
data and ascertained the final histopathology with particular reference to axillary nodal status. Among 449 lesions, AUS
was recorded in 303 lesions (67.5 %). 290 (96 %) were carcinomas, 30.3 % with nodal disease. AUS was abnormal in
46 (15.9 %). AUS had a sensitivity of 39.8 %, specificity 94.6 %, positive predictive value (PPV) 79.2 % and negative
predictive value (NPV) 78.1 %. Axillary FNAB was positive in 27 women, suspicious in two, benign in 16 and not
performed in one. In one FNA positive case, the lesion was a nodular breast primary in the axillary tail in a multifocal
breast cancer. Combining AUS and FNAB, the sensitivity was 76.5 %, specificity 90.9 %, PPV 96.3 % and NPV
55.6 %. Applying the Z0011 inclusion criteria, 24 of the 27 (88.9 %) women with abnormal AUS and positive FNA
were ineligible for Z0011-based management. Of three women eligible for Z0011, one proceeded to AC after SN
biopsy, leaving only two women (7.4 %) who might have been considered for SN only management had it not been for
the results of the axillary assessment. Among women with negative AUS, nodal metastasis was demonstrated in
21.7 %, 86.8 % of these women having only 1-2 positive nodes.
Abnormal AUS and FNA preferentially identify candidates for AC. Negative AUS predicts
negative or low nodal burden. Axillary assessment streamlines care.

PET-TAC
Baseline Tumor 18F-FDG Uptake and Modifications After 2 Cycles of Neoadjuvant
Chemotherapy Are Prognostic of Outcome in ER+/HER2- Breast Cancer.
Groheux D1, Sanna A2, Majdoub M3, de Cremoux P4, Giacchetti S5, Teixeira L5, Espié M5, Merlet P6, de Roquancourt A7, Visvikis D3, Hatt M3,
Resche-Rigon M2, Hindié E8.
J Nucl Med. 2015 Jun;56(6):824-31 This study investigated whether (18)F-FDG PET/CT performed at baseline and during neoadjuvant chemotherapy
(NAC) was able to early depict estrogen receptor-positive/human epidermal growth factor receptor 2-negative (ER+/HER2-) breast cancer patients with
poor clinical outcome.
METHODS:
The NAC regimen consisted of 4 cycles of epirubicin plus cyclophosphamide, followed by 4 courses of docetaxel. The
patients underwent (18)F-FDG PET/CT at baseline and after 2 cycles of chemotherapy. After completion of NAC, all
patients had breast surgery with axillary lymph node dissection. We assessed the impact of 2 PET parameters, maximum
standardized uptake values (SUVmax) and total lesion glycolysis, on event-free survival (EFS).
RESULTS:
Ninety-eight consecutive patients with clinical stage II or III ER+/HER2- breast cancer were included. (18)F-FDG PET/CT revealed distant metastases in
14 patients (14%). Overall survival was significantly shorter in these patients than in the 84 patients classified as M0 at baseline (18)F-FDG PET/CT (P <
0.001). In M0 patients, a high SUVmax at baseline was associated with shorter EFS (P < 0.001). Twelve patients had a tumor SUVmax of 10 or greater
and a 3-y EFS of 49% (vs. 92% in patients with baseline SUVmax < 10). A low change in SUVmax between (18)F-FDG PET/CT examination before
starting NAC and after the second cycle of chemotherapy was also associated with recurrence (P = 0.033), as was a low change in total lesion glycolysis
(P < 0.001). Contrarily to PET-based prediction, the extent of pathologic response after completion of NAC (partial/complete vs. nonresponders) was
poorly correlated to the risk of relapse.
CONCLUSION:
Baseline tumor (18)F-FDG uptake and modifications after 2 cycles of NAC are prognostic of outcome in patients
with ER+/HER2- breast cancer.
Aproximadamente 250 artículos publicados (Junio 2014- Junio 2015)
PET-TAC
Use of [(18)F]-FDG PET to predict response to neoadjuvant trastuzumab and docetaxel in patients with HER2-
positive breast cancer, and addition of bevacizumab to neoadjuvant trastuzumab and docetaxel in [(18)F]-FDG
PET-predicted non-responders (AVATAXHER): an open-label, randomised phase 2 trial.
Lancet Oncol. 2014 Dec;15(13):1493-502
BACKGROUND:
An effective and well tolerated treatment is needed for patients with early HER2-positive breast cancer who do not
achieve a pathological complete response after neoadjuvant therapy. The AVATAXHER trial aimed to predict
pathological complete response early with the use of PET and to investigate whether the addition of bevacizumab
could improve the proportion of patients achieving a pathological complete response in patients unlikely to respond to
treatment.
FINDINGS:
Between May 19, 2010, and Oct 1, 2012, 152 patients were recruited for the study. Ten patients were subsequently excluded, leaving 142 patients in
the intention-to-treat population. Of these 142 patients, 69 were predicted by [(18)F]-FDG PET to be treatment responders after two cycles of
treatment. The 73 predicted non-responders were randomly assigned to group A (n=48) and group B (n=25). Pathological complete responses were
noted in 37 (53·6%, 95% CI 41·2-65·7) of the PET responders, 21 (43·8%, 29·5-58·8) of those in group A, and six (24·0%, 9·4-45·1) of those in group
B. Incidences of grade 3-4 adverse events were similar in all three groups. The most common grade 3-4 adverse events were neutropenia (four in PET
responders, five in group A, and three in group B), febrile neutropenia (one, three, and one, respectively), and myalgia (four, none, and one,
respectively). Overall, 24 serious adverse events were reported in 15 patients (PET responders: nine events in four [6%] of 67 patients; group A: 14
events in ten [21%] of 47 patients; group B: one event in one [4%] of 25 patients). No deaths occurred during the study.
INTERPRETATION:
In patients with HER2-positive breast cancer, early PET assessment can help to identify non-responders to
neoadjuvant docetaxel plus trastuzumab therapy. In these patients, the addition of bevacizumab can increase
the proportion of patients achieving a pathological complete response. This potential new role for PET and the
activity of bevacizumab in this setting need to be confirmed in larger phase 3 trials.