14. manejo terapéutico de lupus eritematoso sistémico y artritis reumatoide
TRANSCRIPT

CURSO DE TERAPEÚTICA MÉDICA
ARTRITIS REUMATOIDEA Y
LUPUS ERITEMATOSO SISTÉMICO
Dr. Julio García Reynoso
Inmunología-Reumatología
Hospital Nacional Arzobispo Loayza

Reumatismos
Afectación
del aparato
locomotor

Sindromes Reumatológicos
• Reumatismos extraarticulares
• Artritis
• Miositis
• Compromiso óseo
• Vasculitis

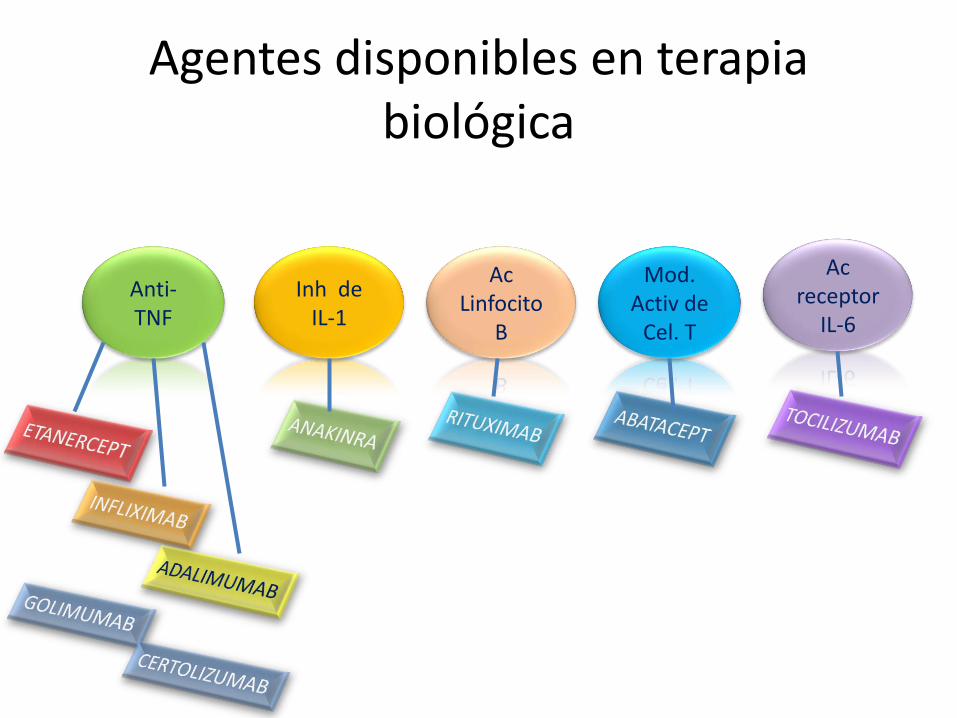
Agentes disponibles en terapia biológica
Anti-TNF
Inh de IL-1
Ac Linfocito
B
Mod. Activ de
Cel. T
Ac receptor
IL-6


ANTI-TNF
• Los tres anti-TNF, anakinra y TCZ tienen la indicación en España de uso como primer biológico en pacientes con fracaso de FAME.
• En estudios controlados de pacientes con AR y respuesta insuficiente al tratamiento con FAME (MTX) los tres anti-TNF, especialmente cuando se combinan con MTX, son superiores a ese fármaco que usado en monoterapia.

• El panel considera que los tres anti-TNF son necesarios y no intercambiables. Aunque ADA y ETN se pueden administrar en monoterapia.
• RTX y ABA están aprobados para pacientes tras fracaso de anti-TNF.
ANAKINRA
• Eficacia inferior a los anti TNF.
• Buena respuesta a la enf. Still.

RITUXIMAB
• Anticuerpo monoclonal contra el CD20 expresada en la superficie de las Cel. B.
• Produce depleción selectiva y prolongada de linfocitos.
• Eficaz en pac. Con fracaso a FAME.
• En combinacion con MTX es superior al MTX en monoterapia.

ABATACEPT
• Interfiere con la señal para activacion de linfocitos T.
• En combinacion con MTX es superior a MTX solo.
• No esta indicado como terapia de primera linea.
TOCILIZUMAB
• Ac monoclonal contra el receptor de la IL-6.
• Eficaz en pac. Con fracaso a FAME y respuesta inadecuada a anti-TNF.

Evaluación clínica, funcional y radiográfica de la AR
Actividad:
• Numero de artic. Dolorosas (NAD) y tumefactas (NAT).
• Valoracion integral de la enf. Escala (0-100).
• Reactantes de fase aguda (VSG,PCR).
DAS 28

DAÑO ESTRUCTURAL
• Evaluacion radiologica que incluya manos y pies, anualmente durante 3-4 años.
FUNCION: HAQ u otros cuestionarios por año.
• El recojo sistematico de las variables permite el calculo de los indices y permite estimar la actividad de la enf: DAS, DAS28, SDAI,CDAI

• Cada decisión terapéutica debe estar precedida por una evaluación objetiva de la actividad de la enf: DAS28 y/o SDAI. Cada 3 meses si no se consigue el objetivo y cada 6 meses si se alcanzo.

OBJETIVO TERAPEUTICO
• Remision de la AR o bajo grado de actividad.
• DAS28 menor 2.6 o 3.2 SDAI menor 5 o 11

CONSIDERACIONES SOBRE EL TRATAMIENTO INICIAL DE AR
• Tratamiento intensivo y precoz mejora la evolucion.
• Alcanzar el objetivo terapeutico lo mas precoz posible.
• Identificar los casos resistentes a terapia inicial.
• El trat. Inicial debe incluir FAME (MTX) administrar a escala rápida hasta 20 o 25 mg/sem en 8 sem.
INDICACIONES DE TERAPIA BIOLOGICA
Elegir en función de :
a. Indicación por ficha técnica.
b. Situación clínica y condiciones generales del pac.
c. Experiencia clínica.

Terapia tras fracaso a FAME
• No se logro el objetivo terapeutico.
• El pac. Recibio FAME MTX o leflunomida en monoterapia o combinacion y a dosis adecuada.
• En caso de suspension de FAME y con respuesta adecuada se recomienda nuevo ciclo antes de TB.

Terapia Biologica de Inicio
• Evaluar posibilidad de iniciar trat. Con anti-TNF o TCZ en combinación con MTX o en monoterapia en caso de CI en quienes se sospecha evolución grave.






Conclusiones
• La preocupación principal del uso de terapias biológicas es el aumento del riesgo de infecciones graves.
• El riesgo disminuye al extremar las medidas preventivas para la infección, especialmente las vacunaciones, la prevención de TBC y evitar los tratamientos concomitantes con glucocorticoides.
• No parece existir mayor riesgo de cáncer ni de mortalidad, relacionada entre otras causas con el beneficio cardiovascular que conlleva el control adecuado de la inflamación crónica.
• La capacidad de inducción de Ac. no se traduce en general en riesgo de enfermedad autoinmunitaria.
• Es preciso ponderar la magnitud del riesgo de reacciones adversas menos graves y frec., como la inducción de psoriasis paradójico, la enfermedad desmielinizante, establecer el riesgo real en embarazos.

Glomerulonefritis Lúpica
Julio García Reynoso
Servicio de Reumatología
Hospital Nacional Arzobispo Loayza

Considerandos
• El compromiso renal es altamente variable.
• Puede ocurrir como una o combinación de los siguientes:
- Nefritis Silente.
- Nefritis Activa
- Síndrome Nefrótico
- Nefritis Rápidamente Progresiva.
- Enfermedad Renal Crónica.
Targered Treatment of the Rheumatic Diseases. Michael H. Weisman et al.
1st edition. Copyright 2010 by Saunders, an imprint of Elsevier Inc.
Inmunología en el diagnóstico de NL
• Systemic markers for SLE activity
anti-DNA antibodies.
C3, C4.
anti-C1q antibodies.
Inmmunology and the diagnosis of lupus nephritis. Philipp Enghard
Lupus 2009: (18): 287-290.

Inmunología en el diagnóstico de NL
• Urinary markers for LN
Proteinuria
Urinary sediment.
Inmmunology and the diagnosis of lupus nephritis. Philipp Enghard
Lupus 2009: (18): 287-290.
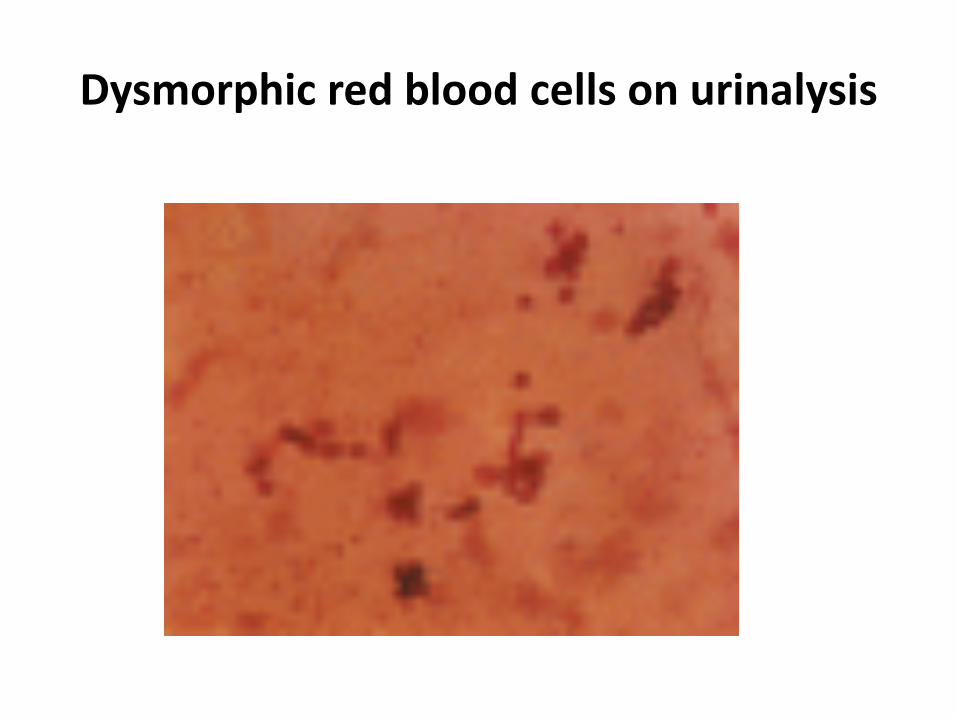
Dysmorphic red blood cells on urinalysis

Hallazgos Sedimento Urinario

Inmunología en el diagnóstico de NL
• Cytokines, chemokines and interstitial infiltration
CXCL10
CXCR3
IL-8
IL-2
IL-4
CD4 T cells and CXCR3 expression Inmmunology and the diagnosis of lupus nephritis. Philipp Enghard
Lupus 2009: (18): 287-290.


Copyright restrictions may apply.
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775
ISN/RPS class IV-Q. The glomerulus shows endocapillary proliferation at the hilum that involves >50% of its surface area, and the uninvolved capillaries are patent

Copyright restrictions may apply.
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775
ISN/RPS class IV-G. There is global endocapillary proliferation involving virtually every capillary in the glomerulus
Copyright restrictions may apply.
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775
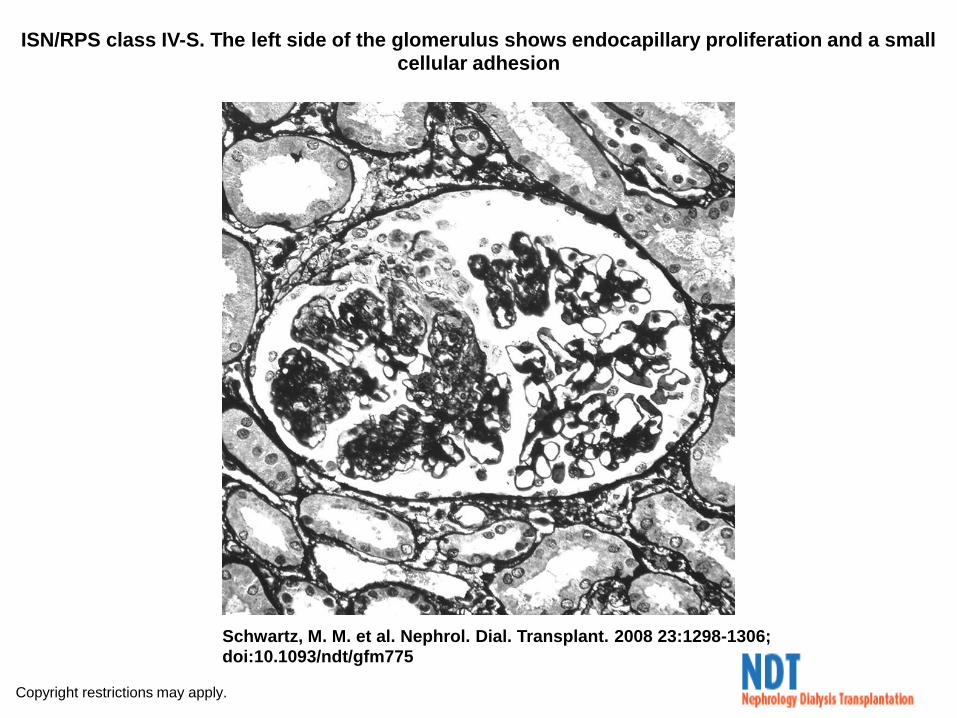
ISN/RPS class IV-S. The left side of the glomerulus shows endocapillary proliferation and a small cellular adhesion
Copyright restrictions may apply.
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775
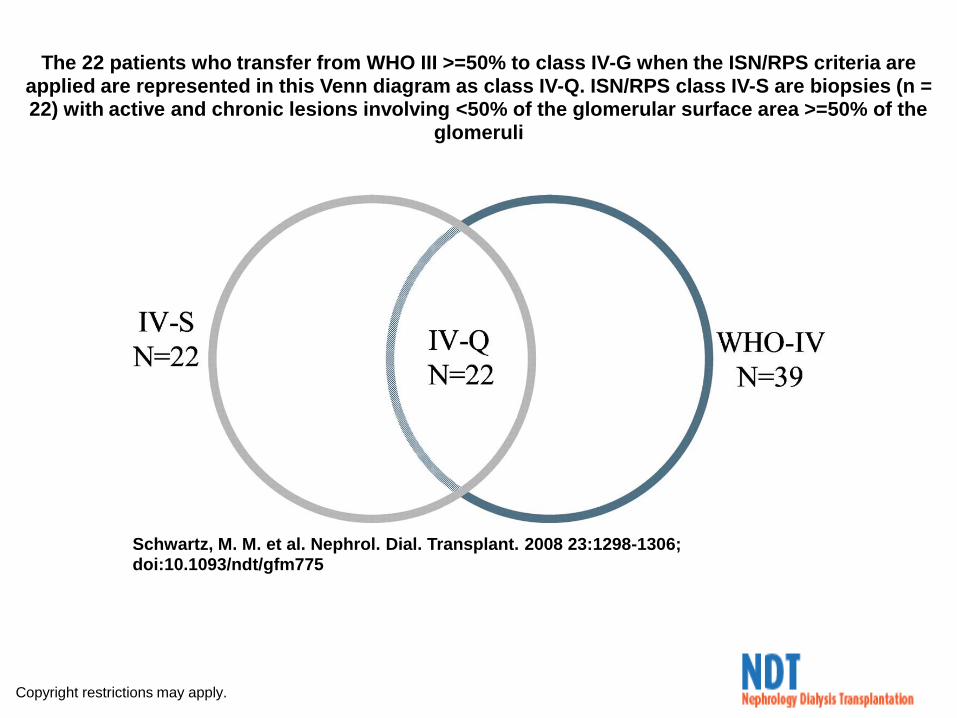
The 22 patients who transfer from WHO III >=50% to class IV-G when the ISN/RPS criteria are applied are represented in this Venn diagram as class IV-Q. ISN/RPS class IV-S are biopsies (n = 22) with active and chronic lesions involving <50% of the glomerular surface area >=50% of the
glomeruli

Características histológicas basales
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775

Características Clínicas basales
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775
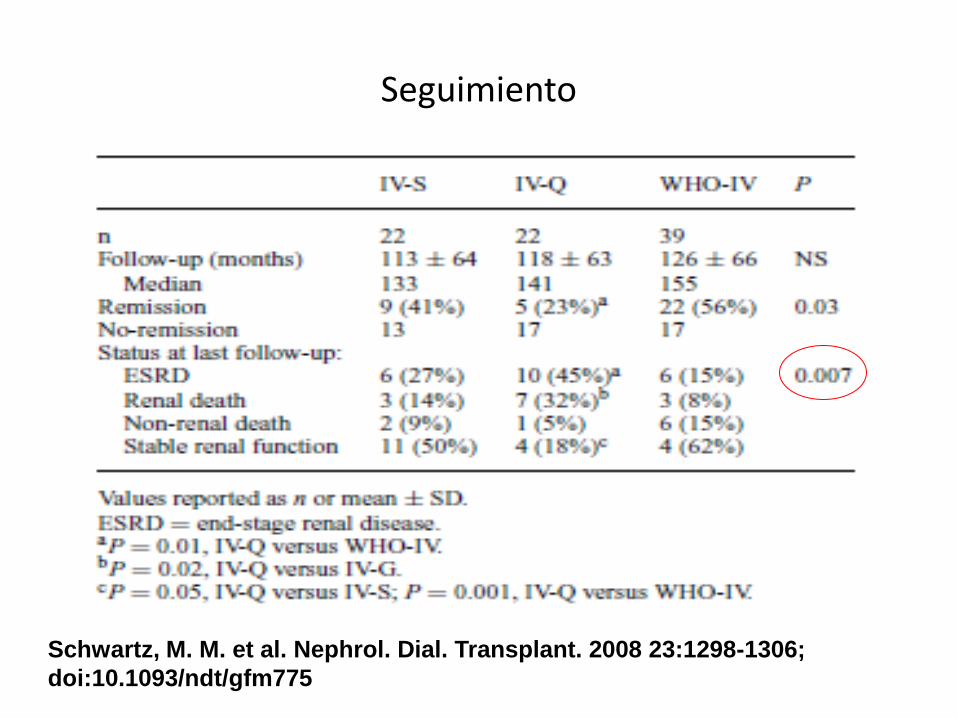
Seguimiento
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775

DIAGNOSTICO
DE ACTIVIDAD
ENFERMEDAD

Copyright restrictions may apply.
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306; doi:10.1093/ndt/gfm775
Patient survival without ESRD
Copyright restrictions may apply.
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775
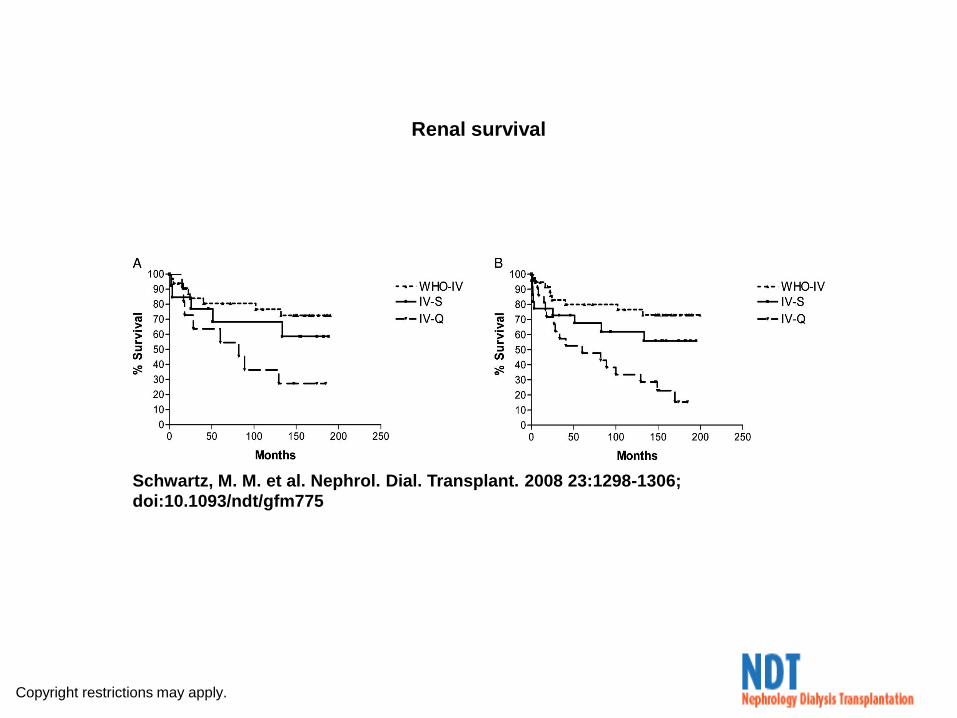
Renal survival

Copyright restrictions may apply.
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775
Renal survival comparing outcome in patients with severe lupus GN
Copyright restrictions may apply.
Schwartz, M. M. et al. Nephrol. Dial. Transplant. 2008 23:1298-1306;
doi:10.1093/ndt/gfm775
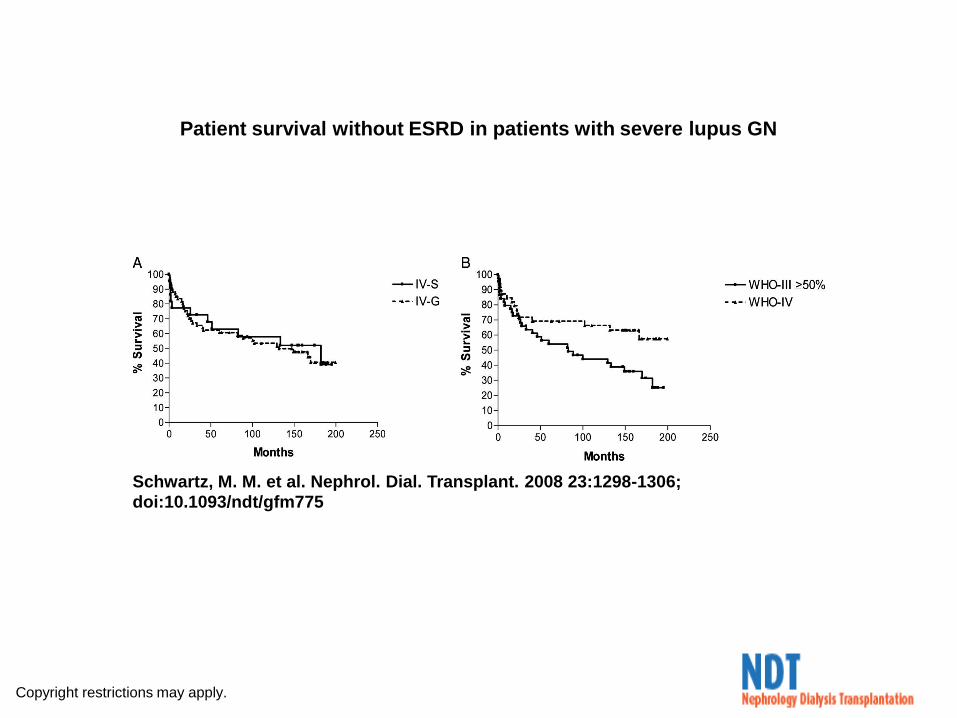
Patient survival without ESRD in patients with severe lupus GN

¿Cuándo hace su efecto?
Cyclophosphamide reaches its peak
effectiveness after approximately
16 weeks.
Clements PJ. Alkylating Agents. In:Dixon J, Furts DE, eds.
Second line agents in the treatment of rheumatic diseases.
New York.1992.

Targered Treatment of the Rheumatic Diseases. Michael H. Weisman et al.
1st edition. Copyright 2010 by Saunders, an imprint of Elsevier Inc.

Efectos adversos