protocolo común para la actuación sanitaria ante la violencia de … · work group protocol and...
TRANSCRIPT

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
Common Protocol for the Healthcare Actions in case of Gender-Based Violence
Commission Against Gender-Based Violence Interterritorial Council of The National Healthcare System
HEALTHCARE
MINISTRY OF HEALTHCARE AND CONSUMPTION

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género

Common Protocol for the
Healthcare Actions in case of
Gender-Based Violence
Commission Against Gender-Based Violence Interterritorial Council of The National Healthcare System
HEALTHCARE
MINISTRY OF HEALTHCARE AND CONSUMPTION

WORK GROUP PROTOCOL AND GUIDE LINES FOR HEALTHCARE ACTION AGAINST GENDER-BASED VIOLENCE
Representatives of the CCAA: Elisa Vizuete Rebollo (Andalusia) José González García (Balearics) Rosa del Valle Álvarez (Canarias) Aurora Rovira Fontanals (Cataluña) Ana Fullana Montoro (Community of Valencia) Jesús Miguel García Ortíz (Extremadura) Mar Martín García (Galícia) José Luis Sánchez Suárez (Madrid) Marina Tourné García (Murcia) Ma.Jesús Ziarrusta Bilbao (País Vasco) Ma.Antonia Aretio Romero (La Rioja) Representatives of other Official Organizations: Carmen Fernández Alonso (SEMFYC) Begoña Merino Merino (General Administration of Public Health. MSC) Begoña López-Dóriga Alonso (Institute of the Woman) Raquel Presa García-López (Special Delegation of the Government against Violence upon the Woman) Health Observatory for the Woman and the National Healthcare System: Concepción Colomer Revuelta Isabel Espiga López Rosa Ma.López Rodríguez Carmen Mosquera Tenreiro Isabel Soriano Villarroel
TECHNICAL SUPPORT:
Juncal Plazaola Castaño (Public Healthcare Andalusian School) Isabel Ruiz Pérez (Public Healthcare Andalusian School)
ACKNOWLEDGEMENTS:
Group of Ethical and Legal Aspects of the Commission against gender-based violence: Jorge González Fernández (Director of the Institute of Legal Medicine of La Rioja) Ma.Luisa Lasheras Lozano (Higher Technician in Public Health of Madrid)
Special cooperation with technical contributions and considerations about the document: Raquel Castillejo Manzanares (Legal Advisor of the Ministry of Justice) Ana Koerting de Castro (National Secretariat of the AIDS Plan) Miguel Lorente Acosta (Medical Examiner) Joaquín Martínez Montauti (Observatory of Bioethics and Right, University of Barcelona) Ana Isabel Vargas Gallego (Attorney Generalship of the State)
INTEGRATED MEMBERS OF THE COMMISSION OF THE INTERTERRITORIAL COUNCIL OF THE SNS AGAINST GENDER-BASED VIOLENCE
José Martínez Olmos (Healthcare General Secretary, MSC) Alberto Infante Campos (General Director of the Quality Agency of the SNC.MSC) Manuel Oñorbe de Torre (General Director of Public Healthcare. MSC) Josefa Ruíz Fernández (Andalusia) Manuel García Encabo (Aragón) José Ramón Riera Velasco (Asturias) Francisca González Porcel (Balearics) Esther Mato Fondo (Balearics) Hilda Sánchez Janariz (Canarias) Santiago Rodríguez Gil (Cantabria) María Alvarez-Quiñones Sanz (Castilla y León) Berta Hernández Fierro (Castilla-La Mancha) Dolors Costa Sampere (Cataluña) Manuel Escolano Puig (Community of Valencia) Pedro García Ramos (Extremadura) Mª Isabel Graña Garrido (Galicia) Mª Belén Prado Sanjurjo (Madrid) José Manuel Allegue Gallego (Murcia) Francisco Javier Sada Goñi (Navarra) Mª Luisa Arteagoitia González (País Vasco) Pilar Díez Ripollés (La Rioja) Vivian Berros Medina (Ceuta) Sara Cristina Pupato Ferrari (INGESA) Concepción Colomer Revuelta (Health Observatory for the Woman. MSC) Rosa Mª López Rodríguez (Health Observatory for the Woman. MSC) Begoña López-Dóriga Alonso (Institute for the Woman) Raquel Presa García-López (Special Government Delegation against Gender-based Violence against the Woman)

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
INDEX PRESENTATION .................................................................................................................. OBJECTIVES AND METHODOLOGY ............................................................................. GENERAL CONCEPTS ……………………………………….…………………………..
1. Definition........................................................................................................................... 2. Causes................................................................................................................................ 3. The process of violence.....................................................................................................
4. Consequences upon health................................................................................................ 5. Importance of the staff of healthcare services................................................................... 6. Difficulties in the identification of gender-based violence................................................ 7. Recommendation for the prevention of violence in the Healthcare system.............................................................................................................. ACTION AT THE PRIMARY AND SPECIALIZED CARE ............................................ 1. Detection and assessment. Procedure algorithm............................................................... 2. Suspicion indicators.......................................................................................................... 3. Identification..................................................................................................................... 4. Assessments......................................................................................................................
5. Action............................................................................................................................... Plan for attention to the woman that shows Indicators of suspicion but that does not.................................................................... Plan for attention to the woman that admits ill-treatment but is not in extreme danger................................................................... Plan for attention to the woman that admits suffering ill-treatment and is in extreme danger........................................................
ACTION IN CASE OF EMERGENCY ............................................................................... 1. Action for violence detection........................................................................................... 2. Action for assistance........................................................................................................ 3. Safety assessment............................................................................................................ 4. Information and derivation.............................................................................................. 5. Legal procedure............................................................................................................... ACTION AGAINST SEX-BASED AGGRESIONS ............................................................ GUIDE TO RESOURCES .................................................................................................... ETHICAL AND LEGAL ASPECTS ..................................................................................... ACTION AGAINST THE ILL-TREATER ........................................................................ REPORT OF DAMAGE AND MEDICAL REPORT............................................................. GLOSSARY OF TERMINOLOGY ..................................................................................... BIBLIOGRAPHY .................................................................................................................. ANNEX: PROTOCOLS AND HEALTHCARE ACTION GUIDE LINES OF THE CC.AA. (AUTONOMOUS COMMUNITIES) .......................................
6
8
10 10 12 13 15 16 18
19
20 21 22 25 28 29
30
31
32
33 33 33 34 34 34
35 41 43 44 45 51 53
57

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
6
PRESENTATION
At the plenary session of the International Council of the National Healthcare System (SNS), celebrated in September 2004, they have agreed to establish a Commission against gender-based violence. It is presided by the Healthcare General Secretary and it is composed of the General Direction of the Agency of Quality of the SNS, the General Secretariat of Policies of Equality and of the Institute for the Woman, the secretariat being in charge of the Observatory of the Health of the Woman. This Commission was gathered for the first time in November 2004. The Organic Law 1/2004 of Measures for Integral Protection against Gender-Based Violence, published in December 2004, in its chapter III establishes that this Commission will give technical support and guide-lines for planning of healthcare measures. Moreover, it will assess and propose the necessary actions for application of the health protocol and of any other measure that may be deemed necessary to contribute to the eradication of this type of violence. It also states that: «The Commission will issue a year report that will be sent to the State Observatory of Gender-Based Violence against the Woman and to the Plenary of the Interterritorial Council»(Art. 16). Moreover the Law through its article 15 establishes that the Healthcare Administrations, in the scope of the Interterritorial Council of the SNS, will promote the action of the professional health officers that allow the early detection of gender-based violence. And will propose the required measures to improve efficiency in the fight against this type of violence, through the development of sensitization programs and continuous training of health officers, which will promote the early diagnosis, the assistance and rehabilitation of the ill-treated woman. Moreover, the Article 32.3 promotes the application, updating, and diffusion of protocols containing homogenised guide-lines for action against this problem.

7
Common Protocol for Healthcare Action against Gende r-Based Violence
Finally, the diagnosis and assistance to gender-based violence, in the scope of primary assistance, as also in the specialized area, are included in the Royal Decree 1030/2006, of September 15th, by which the portfolio of common services of the SNS and the procedures for its updating are established. The Protocol that we are now presenting is the first over this matter that is proposed for application in the aggregate of the SNS. Its objective is to provide the health officers some guide-lines of homogeneous action in cases of violence, specifically addressed against women, in the attention and follow-up, as also in the prevention and early diagnosis. We hope, that will be particularly helpful to professionals of Primary Assistance since at this level more immediate and direct contact with the victim of gender-based violence is established. With this initiative the effort of the SNS to face this problem is enhanced, and the fulfilment of the legal order is accomplished. The Protocol, approved by the plenary of the Interterritorial Council in its meeting of December 2006, has been elaborated by the Commission of the Council against Gender-Based Violence. In order to complete it, the criteria of many experts and the work already done in some of the Autonomous Communities has been taken in account. The work has been elaborate and very participating so that I wish to thank the efforts of all those that have taken part in it.
Elena Salgado
Minister of Healthcare and Consumption
8
OBJECTIVES AND METHODOLOGY
The main objective of this protocol is to establish a normalized and homogeneous guide-line for action, for the National Healthcare System (SNS), concerning so much the early detection as the assessment and action facing the detected cases and their follow-up. The ultimate purpose is to offer guide-lines to the healthcare staff of the SNS for – physical, psychological, emotional and social – integral assistance to women suffering from gender-based violence, that resort to a healthcare centre. This protocol concerns any type of violence and ill-treatment exerted against older than 14-year women, independently whoever the assailant may be, although the actions concerned are more centred in the violence exerted by the intimate partner or former intimate couple, as they are the commonest types of violence in our country. In the case of sex-based aggressions, the assistance and healthcare action is specifical, due to the related measures and medical-forensic and legal implications, so that one chapter related to them, has been included. This protocol has also other secondary objectives :
(1) To sensitize the healthcare staff of the SNS about the seriousness of violence against women as a health problem;
(2) To promote the capability of women suffering ill-treatment to admit their situation and search of solutions;
(3) To contribute from the National Healthcare System (SNS) to sensitize the population in general, about this problem.

9
Common Protocol for Healthcare Action against Gende r-Based Violence
For the elaboration of this Protocol the protocols of healthcare action existing in the CCAA (Autonomous Communities) have been revised. The presented document is the result of the discussion and consensus framed in the Work Group for Protocols and Guide-lines for healthcare action against gender-based violence, originated in the frame of the Commission of the CISNS. The group is compounded with representatives of the Autonomous Communities CCAA and official organisations such as the Special Delegation of the Government against Violence against Woman, the Institute for the Woman (MTAS) and the General Direction of Public Health of the Ministry of Healthcare and Consumption (MSC). For technical support the Andalusian School of Public Health and the Spanish Society for Community and Family Medicine (SEMFYC) have been taken in account. The Coordination of the group has been carried on by the Observatory of the Health of the Woman, of the General Direction of the Quality Agency of the MSC. The Work Group will continue developing the aspects related with the implementation and assessment of the protocol, in the near future.

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
10
GENERAL CONCEPTS
1. Definition
«Any act of violence based in its belonging to the female sex or that may result in sexual or psychological damage or physical suffering for the woman, as also threatening with such acts, coercion or arbitrary deprivation of liberty, as well produced in public life, so as in private life».
(Resolution of the United Nations General Assembly of 1993)
At present, different types of violence against women are defined: Physical violence It contains any non-accidental act that entrails deliberate use of force, such as slaps on the face, blows, beatings, pushes, wounds, fractures or burns, which cause or may cause an injury, damage or pain on the body of the woman. Sexual violence It occurs whenever a sexual behaviour against her will is imposed, be it produced by her intimate partner or by other people. Sexual aggressions comprise any attack against the sexual liberty of another person, exerted with violence or intimidation. Among them is rape: when the sexual aggression consists of penetration with the sexual organ through vaginal, anal or buccal way or the introduction of any type of object or body limb (for example the fingers) by vaginal or anal way. But there is also sexual aggression when there is attack against the sexual liberty of the woman, even when it does not imply any physical contact between her and the assailant (to force her to masturbate or maintain sex relation with third parties). The sexual abuses also comprise any attack against sexual liberty of another person, but carried out without violence or intimidation, but always without consent of that person. Non consented sexual abuses are considered those where consent is obtained when the responsible makes use of a manifest situation of superiority that restrains the liberty of the victim (apart from those exerted upon people less than 13 year old people).

11
Common Protocol for Healthcare Action against Gende r-Based Violence
Within the labour ambit, sexual harassing is also a type of violence against woman. It exists whenever favours of sexual nature are asked from the woman (for himself, or for another one), provoking in the victim an objective and seriously intimidating, hostile or humiliating situation. Offence against sexual liberty and indemnity are typified in the title VIII of Book II of the Penal Laws. There are other types of sex-based violence that are less studied in our country but that cannot be obviated, as for example sexual mutilation, trafficking with young girls and women, sex tourism, among others. These types of violence are also gender-based violence. Psychological violence Wilful and time-prolonged behaviour attacking the psychical and emotional integrity of the woman and also against her dignity as a person, and which objective is to impose the guide-lines of the behaviour that the man considers his intimate partner must exhibit. Its manifestations are threatening, insults, humiliations or vexations, the exigency of obedience, social isolation, inculpation, deprivation of liberty, economical control, emotional blackmail, repudiate or abandon. This Type of violence is not so visible as the physical or sexual one, it is more difficult to prove, and many times it is not identified as such by the victim, but only as the own manifestations of the character of the aggressor. Furthermore, in the case of violence exerted upon women by their intimate partner or former intimate partner, two important elements must be taken in account: the reiteration of the violent acts * and the situation of domination of the aggressor, which exerts violence for the submission and control of the victim . Finally, we must not forget that there are communities of women that because of their personal characteristics or on account of their social or legal situation, are in need of specific attention that give an answer to their specific needs, in order to allow an appropriate follow-up. Such is the case of women with some physical, psychical or sensorial handicap, from rural environment, or w omen in a situation of social exclusion (such as for example women in pros titution or with drug dependency). The vulnerability which prevails in these communities, concerning ill-treatment, imposes to the healthcare staff paying of a special attention.
* Under the present penal regulation of the gender-based violence, the reiteration of violent acts is not
exigible in order to consider as perpetrated an offence of this kind, independently of the fact that such
reiteration might have penal consequences concerning the aggravation of penal liability.

12
Common Protocol for Healthcare Action against Gende r-Based Violence
2. Causes The main factors determining gender-based violence are the unequal relationship among men and women and the existence of the «violence culture», as means of solving conflicts. Violence against women is structural. Violence is not due to singular or pathological traits of a series of individuals, but it has structural traits of a cultural way of definition of the relationship between men and women. Violence against women is exerted in a society the maintains a system of gender relations that perpetuate superiority of men over women and assigns different attributes, roles and spaces as a gender-based function. Up to not many years ago, the restriction on the personal and social development of women, the exigence of exclusive dedication to the family, their duty to obey male authority, were considered something normal and natural, validated by habitude and the law. In this context it was socially tolerated that men exerted violence in order to affirm their authority. At present, there is less social tolerance against violence. However, still too many women bear a high level of violence, so much in their couple-based relationship or from outside it. That happens in all social classes, religions and educational levels. In conclusion, the main risk factor for violence against women is precisely the fact of being a woman. Violence against women is also instrumental. Power of men and subordination of women are that a basic trait if patriarchy, requiring some mechanism of submission. In this sense, violence against women is the means to secure this dominion. Gender-based violence more than a purpose by itself, is an instrument of domination and social control. And in this case it is used as a mechanism of maintenance of male power and reproductions for female submission. Ill-treating men have learnt throughout the socialization process- which is different for women and men-, that violence is the best way to achieve control and dominate the woman. It has been alleged that consumption of alcohol and other drugs is the cause of violent behaviours. Even when consumption of alcohol and other drugs is frequently associated to situations of violence, there are also men that abuse of alcohol and notwithstanding do not manifest any violent behaviour, and many aggressions against women are exerted in absence of alcohol. It has also been alleged that certain personal characteristics of women suffering from gender-based violence might be the cause of ill-treatment. For example, some trends have resorted to characteristics of masochism or pathologies such as hysteria

13
Common Protocol for Healthcare Action against Gende r-Based Violence
or personality dependent disturbance, in order to explain why some women remain or return to a relationship of ill-treatment. At present there is sufficient documented knowledge that shows that there are not any different psychical characteristics before the start of ill-treatment, among women that suffer it and those that do not, but the disturbances and psychological problems of ill-treated women are a consequence of ill-treatment and not its cause.
3. The process of violence
In the case of violence of couple, most frequently ill-treatment starts with behaviours of psychological abuse at the start of the relationship, which are often attributed to zealousness or his zeal of protection of the woman. They use to be restrictive and control behaviours that gradually minimize the decision capacity and autonomy of the woman, producing dependency, isolation and fear, as for example his control of clothing, friendships or activities.
Progressive increase of violence may spread over a long period of time, and it uses to be difficult for the victim to realize the existence of the process in which she is immersed. Leonor Walkers’ s Theory of the Cycle of Violence establishes that this phenomenon comprises three phases:
Accumulation of strain: It is characterized by a progressive raise of strain, where man’s hostility is increasing without any apparent and understandable reason, for the women. They result as isolated episodes that the woman thinks that she can control and will disappear. Tension is raising and accumulating.
Explosion or aggression: Violence outbursts and physical, psychological and sexual aggressions are produced. At this phase is when the woman uses to denounce or ask for help.
Peacefulness, or reconciliation, or honeymoon: In this phase the aggressor manifests that he has repented and asks to be pardoned by the woman. He uses strategies of affective manipulation (presents, caressing, apologies, promises) in order to avoid that the relationship is disrupted. The woman often thinks that all is going to change. As the violent behaviours are establishing themselves and gaining ground, the reconciliation phase tends to disappear and the violent episodes become closer in the time.

14
Common Protocol for Healthcare Action against Gen der-Based Violence However, even when the cycle of violence is very frequent in the relationship of couples where ill-treatment exists, it is not found in all cases. Recently another type of violent relationship has been described where there is a continuous situation of frustration and threat, but only occasionally with appearance of physical aggression. This so-called «moderate form of violence» would be more difficult to be detected than the more severe types of abuse.
ALONG THE PROCESS OF THE VIOLENCE: The woman suffers a progressive loss of self-esteem , and also loses her hope of change of the situation, increasing her submission and fear towards the aggressor. For the ill-treating man it will be the confirmatio n that his strategy works. All that, makes it difficult for the woman t o break their relationship. Because of this, when a woman asks for help, must r eceive in al cases concrete support in order to change her situa tion, respecting and not blaming her for her decisions. It is import ant that she understands that violence will continue and increas e, and that she will not be able to correct the behaviour of her ag gressor, so that se realizes the danger she is in.

15
Common Protocol for Healthcare Action against Gende r-Based Violence
4. Consequences upon health
FATAL CONSEQUENCES Death (through homicide, suicide, etc) CONSEQUENCES UPON PHYSICAL HEALTH Different injuries: bruises, traumatisms, wounds, burns, … that can produce disability Functional deterioration Non-specifical physical symptoms (for example, cephalic pains) Worse state of health CONSEQUENCES UPON CRONIC HEALTH CONDITIONS Chronic pain Syndrome of irritable intestine Other gastrointestinal disturbances Somatical complaints CONSEQUENCES UPON SEXUAL AND REPRODUCTIVE HEALTH Due to forced sexual relations: loss of sex appetite, menstrual disturbances transmission of sexual diseases including VIH / AIDS, bleeding and vaginal fibrositis, dispareunia, chronic pelvic pain, urinary infection, unwanted pregnancy... Due to ill-treatment during pregnancy: vaginal bleeding, threat of abortion, fetal death, early delivery, low weight at birth... CONSEQUENCES UPON PSYCHIC HEALTH Depression Anxiety Sleep disturbances Disturbance due to posttraumatic stress Disturbances of the behaviour of nourishment Suicide attempt Abuse of alcohol, drugs and psychomedication CONSEQUENCES UPON THE SOCIAL HEALTH Social isolation Loss of employment Labour absenteeism Reduction of number of days with healthy life CONSEQUENCES UPON THE HEALTH OF SONS AND DAUGHTERS Danger of disturbance of their integral development Sense of threat Difficulty for learning and socialization doption of behaviours of submission or violence against their male and female companions Higher frequency of psychosomatical diseases Very often they are victims of ill-treatment from their father Transgenerational violence with high level of tolerance in front of situations of violence Violence can also affect other people that depend of the woman , that live together with her

16
Common Protocol for Healthcare Action against Gende r-Based Violence
5. Importance of the healthcare staff From the healthcare service a crucial role can be played in order to help woman that suffer from violence, because the majority of women contact them in some time of their lives (pregnancy, delivery, medical care of their sons or daughters, care of their elder people, etc.). Moreover, ill-treatment affects the health of women so that they resort more frequently to the healthcare service, particularly Primary Attention, Emergencies, Obstetrics and Gynaecology and mental health. The characteristics of this type of violence requires active involvement of the healthcare staff, that will have to be aware of the fact that the approach and solution of the consequences of violence must start with the detection of the problem, even when the victims do not use to manifest or speak about their situation spontaneously. Very often they experience fear, shame, they minimize the seriousness and danger of their situation, they do not admit to recognize it and even they can fall in self-accusation. In many occasions the interdisciplinary intervention with other professionals that not always exist in each primary attention centre, is required, so that the necessary coordination among all involved institutions is needed in order to give an integral and integrated answer to this type of situations. It is difficult to detect ill-treatment when there are no physical injuries. If the healthcare staff is able to deepen with a theurapeutical relation in those psychosocial and gender-based elements that are related to the life style of those that experience it, in their problems and their family situation, one could reach an accurate diagnosis. The detection of the violence situation by the healthcare staff will drive to breaking their silence, which is the first step for understanding and visualising the problem. Non recognizing a situation of ill-treatment as the cause of a health problem, may produce a new victimisation for the woman, that might contribute to the chronification of the ill-treatment and to the medical approach to the problem. As it is stated by the (OMS) World Health Organization in their report about Violence against women. A priority matter, addressed to the healthcare staff: «Do not fear asking. Contrarily to the popular belief, most women are ready to reveal ill-treatment when they are asked in a direct, non valuating way. In fact, many of them are awaiting in silence that somebody asks them». The OMS defines that the minimal functions to be developed in this matter by the Healthcare System are the following:

17
Common Protocol for Healthcare Action against Gende r-Based Violence
To ask regularly, whenever it is feasible, all women about the existence of
domestic violence, as a regular task within the scope of preventive actions.
To be on the watch for eventual signs and symptoms of ill-treatment and follow
them up.
To offer healthcare assistance and register it in the health record or clinical report.
To help understanding their discomfort and their health problems as a
consequence of violence or fear.
To inform and send the patients to the available resources in the community.
To maintain the privacy and confidentiality of the obtained information.
To stimulate and support the woman along the whole process, while respecting
her own evolution.
To avoid non-solidary or blaming attitudes because they may enhance isolation,
undermine their self-confidence and diminish the probability they search for help.
To establish a coordination with other male or female professionals and
institutions.
To cooperate in the assessment and investigation of the problem by registering
the cases.
«Not doing» is to permit that violence continues an d that the health of women gets worse. Acting contributes, to being able to solve the case, and also to the disappearance of the myths and beli eves that concur in gender-based violence. Frequently, one does not ste p in, fearing not knowing what to do, or to cause more harm…, but it is important to state, that the mere fact of listening with respect , is a therapeutic act. Frequently the consultation is the only space for t he woman to talk about what is happening to her. When talking with t he woman one can gradually discover how and in what way she can be h elped.

18
Common Protocol for Healthcare Action against Gende r-Based Violence
6. Difficulties in the identification of gender-based
violence
FROM WOMAN´S SIDE
Fear (the answer of her intimate partner, not to be attended and be blamed, that her confidentiality is not respected, not to be able to start a new life, economical, legal and social difficulties, what is going to happen concerning her children...) Low self-esteem, feeling of culpability To suffer some kind of disability, to be an immigrant, to live in the rural world or in a situation of social exclusion Economical dependence. To be out of the labour market Shame and humiliation Wish to protect her couple Adverseness to recognize what is happening to her Mistrust about the healthcare system Minimizing what is happening to her (sometimes they are not aware of their situation and they find it difficult to identify the danger and deterioration) Isolation and lack of family and social support Values and cultural believes (if society tolerates it, they do too) They are used to hide it Physical and psychological trauma keep them immobilized, baffled, deranged
FROM THE SIDE OF HEALTHCARE STAFF Because they are immersed in the same socialization process as the rest of the society Not considering violence as a health problem Personal experiences concerning vidence Belief the violence is not so frequent Attempt to rationalize the behaviour of the aggressor Double victimization of the woman (the ill-treated woman is blamed for her situation of ill-treatment) Afraid of offending her, worsening her situation, for her safety or for their own integrity Ignorance of the strategies handling these situations Basically biologistical training (not approaching psychosocial problems) Frequent attitudes of paternalism
WITHIN THE CONTEXT OF THE CONSULTATION
Lack of privacy and intimacy Difficulty for communication (for example the language in case of immigrant women...) They come accompanied by their intimate partner. Overload for the assistance. Little training in communication skills at the clinical interview.
WITHIN THE HEALTHCARE CIRCUIT
Lack of knowledge and coordination among the different resources Lack of team work Deficient training over violence

19
Common Protocol for Healthcare Action against Gende r-Based Violence
7. Recommendations for the prevention of violence in the healthcare system
The actions for prevention of violence can be classified in three areas:
PROFESSIONAL :
Including the continuous training of the healthcare staff, aspects about prevention, early detection and integral assistance
Performing interdiscipline sessions about real cases that have been approached in the centre or service
Performing sessions with other male and female professionals and with other institutions
WITHIN THE ASSISTANCE TO THE INTEGRAL HEALTH OF WOM EN:
Informing by placing posters and leaflets in visible places, that show to the women, that violence is a matter of healthcare assistance and to which help can be offered.
Promoting, through the relationship pf the healthcare staff with the patient, attitudes, values and activities that favour the personal autonomy of the woman and performance of her personal, sexual rights, including her social relations.
Including in the activities of training for Health and in the groups of Maternal Education contents of sensitization and prevention of violence against women.
WITHIN THE COMMUNITY CIRCLE:
Cooperating with community associations through workshops, conferences and talks about this violence, explaining the role of the healthcare staff
Proposing and partaking in actions, campaigns, meetings related with this matter, that may be conducting the social institutions and organization.

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
20
1. DETECTION AND ASSESSMENT
Indicators of suspicion Identification Assessment:
Biopschycosocial Of the situation of violence
Of the danger
2. ACTION
Information about the problem Work at the consulting room -follow-up Derivating Recording the clinical report Performance with the sons and daughters (if there are) and with other dependent people if there were
ACTION AT THE PRIMARY AND SPECIALIZED CARE
The primary care teams can take action in the early detection and integral assistance to woman in situation of gender-based violence. The characteristics of accessibility, direct and continued contact with patients and the fact that they can rely on interdiscipline teams can make it easier. Concerning early detection, this protocol states that the healthcare staff must have an attitude of alert at the existence of behaviours, symptoms or signs of suspicion. Furthermore, it is recommended that, in the first examination of each woman, when starting the clinical report, exploratory questions of psychosocial approach be made. When assisting women suffering ill-treatment, further to attention and follow-up of the patient, it is needed, in case of the existence of sons or daughters or other dependant people in charge of the woman, coordination with the paediatric service or with the appropriate services. It is necessary to remember that pregnant women, those with some physical, psychical or sensorial disability, the immigrants, those in a situation of social exclusion or those living in rural environments, are more vulnerable to ill-treatment, for which reason it is necessary to pay them a special attention. The protocol for action is set-up in the following phases:
Issuing the injury report and the corresponding medical report

21
Common Protocol for Healthcare Action against Gende r-Based Violence
1. Detection and assessment.
Procedure algorithm
FIRST CONSULTATION. Opening of clinical report.
Questions for psychosocial
approach : How are things going on at home?. Are you happy with your relations with your
intimate partner and your relatives?
ACTIVE SEARCH at the consultation, concerning indicators of suspicion
(Pag. 24-26)
INDICATORS of suspicion (-)
INDICATORS of suspicion (+)
INVESTIGATE whether she suffers violence
(Pag. 27-29)
The woman does not admit
suffering ill-treatment
The woman admits suffering ill-treatment
Not extreme danger
Extrem danger
WITHOUT PRESENT DANGER
RECORD ON THE CLINICAL REPORT .
Follow-up at the consultation
INTERVENTION PLAN ACCORDING TO
EACH CASE

22
Common Protocol for Healthcare Action against Gende r-Based Violence
2. Indicators of suspicion
There is a series of signs and symptoms that may lead to think that a woman is suffering gender-based violence. It is important that the healthcare staff knows them and maintain an attitude of alert at the consultation in order to identify the cases.
Table 1a. INDICATORS OF SUSPICION IN THE PREVIOUS REPORTS AND CHARACTERISTICS OF THE WOMAN
1. Antecedent of having suffered or witnessed ill-trea tment in her
infancy
2. Personal antecedents and life habits
Frequent injuries Abuse of alcohol and other drugs Abuse of medicaments, especially psychomedicaments
3. Gynaeco-obstetrical problems
Inexistence of fecundity control (many pregnancies, unwanted or non-accepted pregnancy)
Presence of genital injuries, abdomen or breasts during the pregnancies Dispareunia, pelvic pain, repeated gynaecological infections, anorgasmy, dysmenorrhoea Record of repeated abortion Children with low weight at birth Delay in her request for prenatal attention
4. Frequent psychological symptoms
Sleeplessness Depression Anxiety Posttraumatic stress disturbance Suicide attempts Low self-esteem Physical exhaustion Irritability Disturbances of nourishing behaviour Emotional lability
23
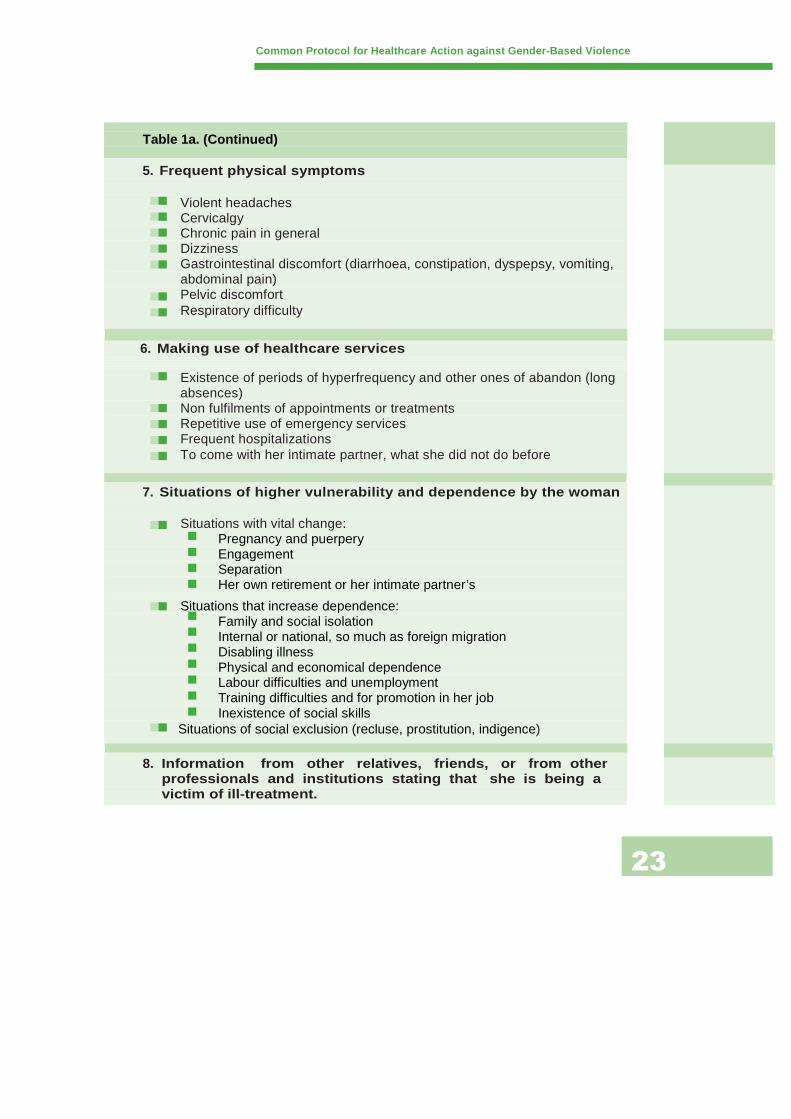
Table 1a. (Continued)
5. Frequent physical symptoms
Violent headaches Cervicalgy Chronic pain in general Dizziness Gastrointestinal discomfort (diarrhoea, constipation, dyspepsy, vomiting, abdominal pain) Pelvic discomfort Respiratory difficulty
6. Making use of healthcare services
Existence of periods of hyperfrequency and other ones of abandon (long absences) Non fulfilments of appointments or treatments Repetitive use of emergency services Frequent hospitalizations To come with her intimate partner, what she did not do before
7. Situations of higher vulnerability and dependence b y the woman Situations with vital change:
Pregnancy and puerpery Engagement Separation Her own retirement or her intimate partner’s
Situations that increase dependence: Family and social isolation Internal or national, so much as foreign migration Disabling illness Physical and economical dependence Labour difficulties and unemployment Training difficulties and for promotion in her job Inexistence of social skills
Situations of social exclusion (recluse, prostitution, indigence)
8. Information from other relatives, friends, or from other professionals and institutions stating that s he is being a victim of ill-treatment.
Common Protocol for Healthcare Action against Gende r-Based Violence

24
Table 1b.
INDICATORS OF VIOLENCE, DURING THE CONSULTATION
1. Characteristics of the injuries and health problems
Delay in the request of assistance for physical injuries Incongruence between the type of injury and the explanation of their cause Haematomas or bruises in suspicious areas: face/head, interior side of arms and thighs Injuries because of defence (interior side of forearms) Injuries in different stages of treatment that indicate violence of long time of evolution Injuries in the genitals Injuries during pregnancy, in genitals, abdomen and breasts Typical injury: rupture of tympanum
2. Athitude of the woman :
Fearful, evasive, uneasy, nervous, disturbed, for example, when the doors opens… Depressive traits: sad, lack of motivation, disilluded, hopeless Low self-esteem Feeling of culpability Condition of anxiety or anguish, irritability Feeling of shame: reclusion, difficult communication, avoiding looking in the face Clothing that may indicate the intention to hide injuries Lack of personal care She justifies her injuries or obviates their importance: If her intimate partner is present
She is fearful in her answers She is constantly looking for his approval
3. Attitude of her intimate partner
He asks to be present along the whole of the consultation Very controlling, he always answers, or, on the contrary, careless, depreciatory or trying to trivialize the facts Exceedingly worried or solicitous towards her Sometimes angry or hostile against her or the professional.
Common Protocol for Healthcare Action against Gende r-Based Violence
25
Common Protocol for Healthcare Action against Gende r-Based Violence
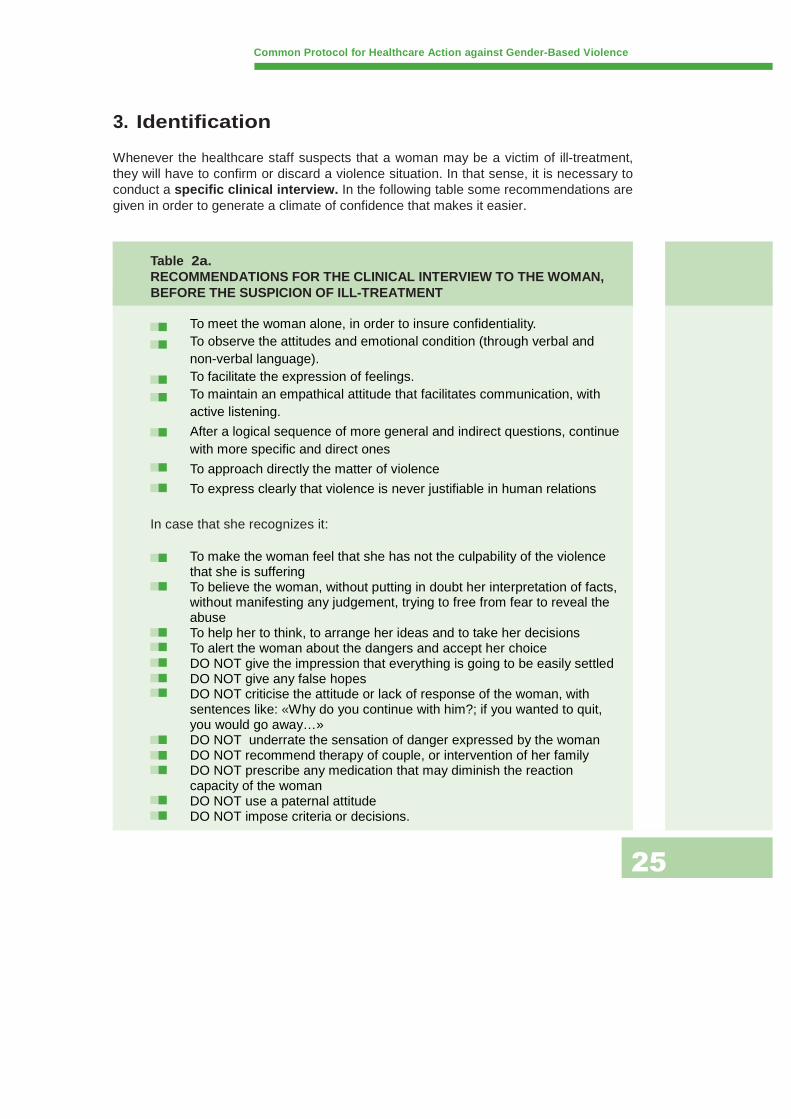
3. Identification
Whenever the healthcare staff suspects that a woman may be a victim of ill-treatment, they will have to confirm or discard a violence situation. In that sense, it is necessary to conduct a specific clinical interview. In the following table some recommendations are given in order to generate a climate of confidence that makes it easier.
Table 2a. RECOMMENDATIONS FOR THE CLINICAL INTERVIEW TO THE W OMAN, BEFORE THE SUSPICION OF ILL-TREATMENT
To meet the woman alone, in order to insure confidentiality. To observe the attitudes and emotional condition (through verbal and non-verbal language). To facilitate the expression of feelings. To maintain an empathical attitude that facilitates communication, with active listening.
After a logical sequence of more general and indirect questions, continue with more specific and direct ones
To approach directly the matter of violence
To express clearly that violence is never justifiable in human relations
In case that she recognizes it:
To make the woman feel that she has not the culpability of the violence that she is suffering To believe the woman, without putting in doubt her interpretation of facts, without manifesting any judgement, trying to free from fear to reveal the abuse To help her to think, to arrange her ideas and to take her decisions To alert the woman about the dangers and accept her choice DO NOT give the impression that everything is going to be easily settled DO NOT give any false hopes DO NOT criticise the attitude or lack of response of the woman, with sentences like: «Why do you continue with him?; if you wanted to quit, you would go away…» DO NOT underrate the sensation of danger expressed by the woman DO NOT recommend therapy of couple, or intervention of her family DO NOT prescribe any medication that may diminish the reaction capacity of the woman DO NOT use a paternal attitude DO NOT impose criteria or decisions.

26
Common Protocol for Healthcare Action against Gende r-Based Violence
In the Table 2 b. examples of general questions are given that might be used at the consultation for active search of ill-treatment cases, in case of suspicion.
Table 2b. EXAMPLES OF QUESTIONS IN CASE OF SUSPICI ON
In case of suspicion obtained from antecedents and characteristics of the patient :
I have gone through your file and find some things that I would like to comment with you. I see that…(report your findings), what do you think your discomfort or health problem is due to?, I find you a little uneasy, what worries you? Are you experiencing any problematical situation that makes you feel so?, what can you tell me? Do you think that all this is interrelated?
In many cases in women with problems like yours, such as …(report some of the identified ones, the most significative), they use to be caused because they are receiving some type of ill-treatment from somebody, for example, their intimate partner, is that your case?
In case of suspicion from antecedents, such as dispareuny, pelvic pain… ask whether her affective and sexual relations are satisfactory or not
In case of suspicion from the exhibited injuries :
This injury uses to appear whenever a push, blow, cut, punch, has been received…is that what has happened to you? Your intimate partner or another person uses force against you? How? Since when? Have you been more seriously aggressed any time? (beating, use of weapons, sexual aggression).
In case of suspicion because of the symptoms or psy chical problems found :
I would like to know your opinion about those symptoms that you have explained (anxiety, nervousness, sadness, apathy…): since when do you feel so?, what do you think they are due to?, do you relate them to something? Anything has happened in your life that keeps you worried or sad? Have you perhaps any problem with your intimate partner? Or with your sons or daughters? With somebody in your family? In your job? It seems that you are alert, afraid, what do you fear? Have you any difficulty to meet your friends or relatives? What is hindering you to do it?

27
Common Protocol for Healthcare Action against Gende r-Based Violence
Table 2c. QUESTIONS IN ORDER TOASSESS THE SITUATION AND TYPE OF VIOLENCE
Physical violence
Does your intimate partner push or grip you?
Does your intimate partner beat, slap or aggress you in any other way?
Sexual violence
Does your intimate partner force you to maintain any sexual intercourse that you do not want? Does he force to carry on any sex practice that you do not wish?
Psychological violence
Does he often shout at you or in a domineering way?
Does he threaten to harm you, your daughters and sons, other people, or domestic animals?
Does he insult, laugh at or underestimate you, when alone or in front of other people?
Does he become zealous without any reason?
Does he impair or make it difficult for you meeting your family or friends?
Does he blame you for all what happens?
Does he control your money and compels you to submit an account of your expenses?
Does he prevent you from working outside the home, and from studying?
Does he threaten you to take away your sons or daughters if you abandon him?
Does he not want to know about your feelings, if you are present, etc?

28
Common Protocol for Healthcare Action against Gende r-Based Violence
4. Assessments
Once the woman has recognized that she is in a situation of ill-treatment, one must conduct an exhaustive exploration of the injuries and her emotional condition, informing her about the conducted explorations and their purpose.
Table 3. ASSESSMENTS
BIOPSYCHOSOCIAL
Injuries and physical symptoms Family situation Economical, labour and occupational situation Social support net of the woman Emotional condition
ABOUT HER SITUATION OF VIOLENCE
Type of violence, since when she is suffering from it, frequency and intensity of the same Behaviours of the aggressing person at family and social level, if there have been aggressions to other people or relatives Mechanism of adaptation developed by the woman Stage of the process of violence where she is in
ABOUT SAFETY AND ASSESSMENT OF THE RISK
To determine whether the woman is in an extreme danger, being understood as an extreme danger the present situation of an imminent event with a real danger for the life of the woman or that of her sons or daughters. Indicators of extreme danger. This assessment will be made together with the woman:
Threatening with weapons or use of the same Threatening with homicide attempts to them and their sons or daughters Threatening with suicide attempts from the patient Ill-treatment to sons or daughters or to other members of the family Serious injuries, even requesting hospitalization Threating or harassing, even being separated Increase of intensity and frequency of the violence Aggressions during pregnancy Repeated sexual abuse Violent behaviour outside home Extreme zealousness, obsessive control of her daily activities, where she goes, with whom she is, how much money she has Increasing isolation Consumption of alcohol or drugs by her consort Decrease or absence of remorse expressed by the aggress
To consider the awareness of danger by the woman, so much for her as for other members of the family environment. At the existence of this indicator, the situation is directly defined as extreme danger. Professional judgement after the joint assessment (basically during the interview and the conducted biopsychosocial assessment) If a situation of danger is detected, ask:
Do you feel safe at home? Can you go home now? Are your children safe? Where is now the aggressor? Do your friends or familiars know about it? Would they help you?

29
Common Protocol for Healthcare Action against Gende r-Based Violence
5. Action
The confirmation of the suspicion of ill-treatment to a woman does not stop the action of the healthcare staff, but from these moments on an important work of information to the woman, of assistance and work at the consultation must be developed, as also derivation when the characteristics of the case require it. The action of the healthcare staff will be different if the woman recognizes or not, ill-treatment and depending on the situation of danger she is in. This, 3 possible situations arise from which different guide-lines for action will have to be planned:
Woman that it is suspected that she is suffering il l-treatment
Woman that recognizes she is suffering ill-treatmen t but is not in extreme danger
Woman that recognizes she is suffering ill-treatmen t and is in extreme danger.
.

30
Common Protocol for Healthcare Action against Gende r-Based Violence
Plan for assistance to the woman that presents indicators of suspicion but does not recognize to be suffering ill-treatment
Record in the clinical report the suspicion and the conducted action To inform the woman of the situation she is in Work at the consultation – follow-up :
Integral / interdisciplinary attention Assistance for the physical / psychical / social problems found To offer follow-up visits: to accompany the woman in the recognition of the situation of violence and in taking decisions, in an empathic way To offer, if it is possible, the participation in group interventions (groups of women inside the centre or in other resources in the area)

31
Common Protocol for Healthcare Action against Gende r-Based Violence
Plan for assistance to the woman recognizes to be suffering ill-treatment, but is not in
extreme dange
Record the clinical report Inform the woman about the situation she is in Work at the consultation – follow-up :
Integral / interdisciplinary Assistance
Assistance for the physical /psychical / social problems found
Planning of a safety strategy before an eventually extreme situation
To establish planning of consultations and follow-up for:
Stating and promoting taking decisions to start changes in the situation To accompany the woman to face her situation To prevent new situations of violence To offer, if possible, the participation in group interventions (groups of women inside the centre or other resources in the area).
Derivate (if it is deemed necessary and with previous consent of the woman)
Towards the social work staff Towards the appropriate resources for the situation the woman is inç
To issue an injure report when it is needed *
Action with the sons and daughters and other dependent people, if there were
* In those cases that the woman rejects to report, but the healthcare staff have basic suspicion of the existence of physical or psychical ill-treatment (the origin of the injuries is not clearly established for the corresponding injury report to be issued), it is recommended to inform the Attorney-Generalship about this situation, as it is established in the legal prescription. The Attorney-Generalship will decide, based upon the evidence that can be given or extended, which is the appropriate legal situation.

32
Common Protocol for Healthcare Action against Gende r-Based Violence
Plan for assistance to the woman that recognizes to be suffering
ill-treatment and is in extreme danger
To inform her about the situation of danger she is in and state eventual strategies to be followed. To transmit to her that she is not alone. To derivate, with urgent character, towards social work or to the support services of the 24-hour soci al emergencies for women that suffer ill-treatment To file in the clinical report the episode and the actions taken. This record can be used as a proof i n judicial proceedings To issue an injure and medical report handing a cop y to the woman and informing her about its implicatio ns To know about the family situation, dependent peopl e and resourced that she has. To call the 112 ( Emergencies) or to the specific services of her autonomous community

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
33
ACTION AT EMERGENCIES
Women suffering gender-based violence can also resort to the emergency services, so much in the scope of primary assistance as the specialized one. Most of the actions, stated in the previous chapter might also be recommended for emergencies, with the exception of the actions concerning follow-up at the consultation. At the emergency service the injuries and symptoms of the patients frequently are more serious. The women that resort to emergencies for this problem, may recognize having received ill-treatment, or not.
1. Action for detection of violence
To maintain an attitude of alert and pay attention to signs and symptoms that might induce to think that the patient suffers ill-treatment. (Indicators of suspicion. Table 1 b. Page 24) In cases when that is suspected, conduct a specifical clinical interview in order to detect ill-treatment. (Identification. Table 2 b. Page 26) To assist the woman in an appropriate climate of confidence. (Identification. Table 2 a. Page 25)
2. Action for the assistance
In the first place, the health condition of the woman must be attended, physical and psychological condition, and establish a diagnosis and appropriate attention. The attention to the patient will be according to the injuries and symptoms exhibited, and in case that hospitalization is not necessary, the need of urgent action by psychology / psychiatry and social work professionals will be assessed. Also, the existence of minors or dependent people that might also be suffering violence must be searched, for immediate measures that may have to be taken. The discharge report that is handed to the woman, must state the injuries that she presents and her psychological condition. It must be delivered to the woman whenever it does not threaten her own safety (she may come accompanied by the alleged aggressor or maybe that when arriving home the aggressor may discover

34
Common Protocol for Healthcare Action against Gende r-Based Violence
the copy of the discharge report). In that case, one may advise that if she fears to carry the copy along with her, she can hand it to some familiar or a person she can trust. Another copy will be for primary assistance, in order to cooperate in her follow-up and to complete the actions that might be needed. .
3. Assessment of the safety
Whenever a case of gender-based violence is attended at emergencies, it is needed to conduct an assessment of the safety and the danger the woman is in (assessments. Table 3. Page 28).
4. Information and derivation
After fulfilment of the assistance and care matters, the appropriate informative and derivative actions according to the case, will be made.
5. Legal action
In Spain there is the legal obligation to inform the judicial authority about the existence of injuries in case of proven ill-treatment, this obligation being accomplished by means of submitting to the court the injury report and the adjoining of the medical report, having previously informed the affected woman about its remission and recording it in the clinical report.

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
35
ACTION IN CASE OF SEXUAL AGGRESSIONS
The procedure for action in case of sexual aggressions has certain particularities that justify its being described in an independent section. The definitions of these cases are gathered in the pages 10-11.
Sexual violence against women can be exerted by their intimate partner or by other men. In general, women consult when the aggressor is not her intimate partner, and it is not often that they do it because of sexual aggression within the couple. It is in these last cases when sexual violence uses to remain hidden, and it is difficult to detect. The sanitary staff of Primary Care or other non-hospital service, that attend sexual aggression, excepting supposition of seriousness and vital risk that compel to immediate medical treatment, will send the victim to the closest hospital as soon as possible in an ambulance, without practicing any cleaning or changing of clothing. In case of fellatio it is important, as much as possible, to avoid the intake of food or liquids before the examination of the victim in hospital. It is necessary to promote an empathic treatment to the woman, by enabling an atmosphere that favours the communication, confidentiality and the greatest possible intimacy. If the victim wishes, some trusty person may be present. Jeopardizing questions must not be made, only collecting the facts that the woman wishes to give. It is a must to inform the woman about all the explorations that are going to be made and their purpose, and commenting all the time what is being done, and asking for consent when necessary. Concerning this matter it is evident that the psychical impacts that the woman is going to suffer after the aggression must be reduced to the least possible. For that reason, it is not only justifiable, but even recommendable that the gynaecological and the medical forensic assessments are conducted in one simple action, with independence between the sanitary and legal expert actions, but trying that no new examinations are needed. For that reason, since there is no legal or ethical constraint –rather on the contrary- in order that the examinations in case of sexual aggressions are made in a simultaneous and coordinated way, immediate communication is needed, though

36
Common Protocol for Healthcare Action against Gende r-Based Violence
the telephone with the Police Court that will agree the attendance of the forensic doctor and will commend the duty doctor to collect the specimen of legal interest*. The general actions depending on each professional, in these cases, are stated below:
Actions from the clinical medicine :
o To conduct the anamnesis and the clinical examination o To ask for the action of the forensic medicine through the police court,
and cooperate in their work. o To take specimen from her genital parts, in search of infections from
sexual transmission o To ask for blood analysis to be conducted o Immediate treatment of eventual physical injuries o Treatment of sexual transmission infections o Pregnancy prophylaxis o To issue a report of the injuries
Action from the forensic medicine :
o Taking of specimen of legal interest** o To spot the location and importance of the injuries (to take
photographic pictures of the injuries) o To issue the Forensic Medical Report for the Court
In the following tables, the actions to be conducted by the Emergency Services in cases of sexual aggressions are described in detail:
* For penal proceedings against offence for sexual aggressions, the formal report made by the damaged person, her legal representative or complaint brought by the District Attorney will be needed, (when the victim happens to be a minor, unable or a disabled person, with the complaint by the District Attorney will be sufficient). Even when the woman stated that in that moment she does not want to report a complaint, the facts must be communicated to the Police Court, so that they can commence legal proceeding, having the required investigation and security means so that the remaining of the legitimate, or the own woman, in the future, might wish to commence a penal procedure.
** The National Institute of Toxicology and Forensic Sciences, and the Institute for the Woman, cooperating with the Centre of Judicial Studies of the Ministry of Justice, have introduced in several provinces and Autonomous Communities a “kit” for taking specimen in cases of sexual aggressions. It contains the whole of a set of instruments for the correct taking of specimen (hyssops, nail scissors, combs, bags, labels…). Further to this set of instruments, it also contains a series of elements that contribute to the environment when the examination is to be made, by conferring to it intimacy and dignity that in these cases is much needed in order to diminish the risk of secondary victimization. .

37
Common Protocol for Healthcare Action against Gende r-Based Violence
RECORDING IN THE CLINICAL REPORT
It can be used as an important proof in the legal procedure
To transcribe the facts stated by the patient, concerning the aggression (date, place, time, type of sexual aggression) and the actions carried out after the aggression and before the examination (personal hygiene, intake of food or medication etc)
Antecedents of diseases, interventions, medication, associated consumption of alcohol and other drugs, etc.
Antecedents of violence, in case there were
Gynaecological report: menarche, menstrual period, date of the last period, contraceptive method, last sexual intercourse.
EXAMINATION (GENERAL AND GYNECOLOGICAL )
Examination of body surface :
Explain in detail location and importance of injuries (wounds, bruises, erosions, lacerated wounds), and also stating non-existence of them. In case they are present it is convenient to take pictures, with previous consent of the woman
Specimen with legal interest :
To take semen, blood specimen or of other fluids on the body surface, by means of sterile hyssop slightly moistened with distilled water, placing the specimen in a tube to be sealed, labelled and maintain it cooled (4-8 ºC).

38
Common Protocol for Healthcare Action against Gende r-Based Violence
EXAMINATION (GENERAL AND GYNECOLOGICAL) (continued… )
Gynaecological examination:
Vulvo-vaginal inspection: detail injuries, haematoma, bruises, and if not so, stating their non-existence. In case of sexual aggressions against women that have not had any previous intercourse, it is interesting to state the eventual existence and location of hymen laceration, which shows the existence of penetration.
Bimanual tactile test: in order to assess size, shape, consistency and uterine mobility, as also the eventual existence of mass aggregations or annexial pain. An echography may be eventually needed.
Specimen of legal interest : Vaginal (or anal or buccal) intake of specimen, by means of dry and sterile hyssop for investigation of sperma. They will be kept in their sheath without inclusion of any preserving stuff, it will be kept cooled (4-8 ºC) and will be labelled. It is recommended to make the intakes with at least two hyssops. Vaginal (or anal or buccal) cleaning with 10 cc of sterile physiological serum to collect eventual remnants o semen. The cleansing liquid will be collected in an appropriate sterile tube that can be hermetically sealed and will be labelled. It will be kept cool (4-8 ºC). Vaginal cleaning will be after the intake of specimen for screening of sexual transmission infections. Clothing of the victim concerning the presumptive aggression, place each piece of clothing in an independent bag, which will be labelled. Intakes moistened with physiological serum hyssop in case of anal or buccal aggression, from the concerned cavities, and placing the hyssop in a tube, for sealing and labelling. Scraps of nail cleansing (eventual presence of skin of the aggressor). Combing of pubic hair of the aggressed woman (eventual hair of the aggressor).
Labelling of the specimen will contain the name of the patient, date and signature of the professional. The different specimen will be introduced in an envelope with the name of the woman and will be sent to the forensic medicine of the Police Court. In case that the intake of the specimen has not been conducted by the Forensic Surgeon, the custody chain must be insured so that the obtained specimen have any legal value, that is, the responsible of the intake and the one for transport of it up to the forensic-medical service of the Police Court must documentarily state their identity, the exact statement of the obtained and sent specimen, and leaving evidence of the person whom the specimen are delivered in the forensic-medical premises.

39
Common Protocol for Healthcare Action against Gende r-Based Violence
ANALYSIS
To determine blood group and Rh of the patient
Test for toxic substances
Pregnancy test
Sexual transmission infections: Culture early diagnosis, gonorrhoea and Chlamys: initial and after 7 days. Syphilis: initial and after six weeks. VIH: initial, after six weeks, and after 3 and 6 months. Hepatitis B: initial and after six weeks.
Cytological smear, also useful for moniliforms and trichome
ATREATMENT AND FOLLOW-UP
Treatment of physical injuries and psychological s equel Physical traumatisms: treatment of the wounds and contact prevention of their infection, and if necessary, prophylaxis of tetanus. Psychological traumatisms: in general, it consists in derivating in a preferent mode, the woman, to a psychical or psychological consultation. In general, women having suffered sexual aggression have a feeling of anxiety, culpability, humiliation, shame, which has to be treated.
Prevention of sexual transmission infections : Preventive treatment must be used against gonococcus, chlamys and syphilis in eventual incubation.
The need of prophylaxis against VIH: the risk of transmission of VIH is high if the aggressor is VIH+, suffers from other sexual transmission infections and there was ejaculation. Consider prophylaxis following the recommendation about non-occupational post-exposition prophylaxis.
Need of prophylaxis against the virus of Hepatitis B is to be individually assessed.
Pregnancy prophylaxis : In case that the woman is using an effective contraceptive method, prophylaxis is not needed.
Hormonal post-intercourse contraception, if less than 72 hours have elapsed after the aggression.
If more than 72 hours, but less than 5 days have elapsed after the aggression, the previous method is not deemed effective and an Intrauterine Device must be placed.
Confirm the next menstruation or conduct a pregnancy test after 2-3 weeks.
To inform the woman that in case of pregnancy she may opt for its interruption according to the legal terms.

40
Common Protocol for Healthcare Action against Gende r-Based Violence
INFORMATION AND DERIVATION
To inform the woman about :
Sexual aggression is a delict and the woman has the right to report it. Analyze together with her the repercussions on physical and emotional health. To inform her that the legislation protects her rights and integrity and if she wishes she can apply for Protective Custody. To inform her about the net of resources and social devices (preferably in writing) for assistance to women suffering from gender-based violence), according to their organization in her Autonomous Community or province.
Derivation :
Importance of derivation to/ and coordination with primary healthcare and social work, insuring the psychological, social and juridical attention for the woman, according to the organization and own resources of her Autonomous Community or province.
RECOMMENDATIONS
No sexual intercourse till the next assessment
Appropriate follow-up of the whole process of integ ral attention of her health
NOTIFICATION TO THE COURT
To issue the report of injuries and medical report for the police court *.
(*) In the medical report must be included the results of all the conducted and recommended medical tests of this protocol.

41
GUIDE-LINE FOR RESOURCES
As it has been repeatedly stated along this protocol, the coordination and intersectorial cooperation (with social, juridical, police, etc resources) is essential in the attention to woman suffering ill-treatment. It is important that each professional knows about the specific resources that are available at national, autonomy, provincial and municipal level, and their characteristics, with the purpose of facilitating the appropriate use. In that sense, the professionals of social work represent a linking figure that is essential in the process of derivation of the women. It is also important to bear is mind that derivation to a resource must not be considered as the end of the action, and that follow-up of the women at the consultation is also essential. In this chapter, only the resources at national level are detailed, since in each Autonomous Community there are a lot of them, including those of provincial and municipal range. For this reason, this part of the protocol has to be adapted to the characteristics of each Autonomous Community.
RESOURCES AT NATIONAL LEVEL
Telephones for 24-hour information of the Institute for the Woman:
900 191 010 900 152 152 (for deaf women)
Service of Attention to Urgencies and Emergencies: 112 National Police: 091 Civil Guard: 062 Special Government Delegation facing Violence against Women
91 363 52 53 / 54
http://www.mtas.es/igualdad/violencia.htm All the telephones shown are free .

42
Common Protocol for Healthcare Action against Gende r-Based Violence
Below, a generic list of resources is presented, so that the different Autonomous Communities show their addresses and telephones of each one. The resources for emergency cases must be distinguished from the non-urgent ones.
RESOURCES IN THE AUTONOMICAL COMMUNITIES
Service for Attention of Urgencies and Emergencies in the Autonomous Community.
SAM (Service of Attention to the Woman, of the National Police) in the Autonomous Community.
EMUME (Woman-Minors specialists of the Civil Guard) in the Autonomous Community.
Municipal Police.
Reports to the police, application for protective custody and to the service of mobile teleassistance: for the National Police, Municipal Police, Civil Guard, Police Stations (a list of them), Prosecutor’ s Office (address and telephones).
Guidance and Judicial consultancy (detail the addresses and telephones):
Telephone 900 of the Autonomous Community (if there are) Service of Judicial Guidance of the College of Lawyers Equality organizations of the Autonomous Communities Social Services of the Town Councils Service of Attention to the Victims of Violent Offences and Against Sexual liberty, in the Courts Women Organizations Immigrant Organizations (especially important to show those that assist immigrants whose language is not Castilian).
Shelter houses: information in Equality Organizations of the Autonomous Communities and Social Services of the Town Councils (reflect only that, do not show a list). If there are specific programs about gender-based violence, they should be stated. Any other resource of the Autonomous Community that is specific for this matter.

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
43
ETHICAL AND LEGAL ASPECTS
When taking decisions at the consultation, for a situation of ill-treatment, the healthcare staff must take in account, that among their tasks there is offering listening and support, and to respect the decision of the woman. Many of the women, even when they present important injuries, do not resort to the sanitary services because of shame, being threatened by the aggressor or because they fear that may be communicated to the court the origin of their injuries and measures might be taken that could affect their family. During the process of attention to the woman that may be suffering gender-based violence, it is important to respect the autonomy of the patient and the compromise of confidentiality concerning the information being learnt by virtue of professional praxis. It is also important to look after the life and the benefit of the health of the patients (principle of beneficency) and avoid harms for the health (principle of maleficence). In case of confirmation of ill-treatment situation, it will be notified to the Court for gender-based violence by means of the report of injuries and the medical report, having previously informed the woman. The information of the facts to the judicial authorities allows the start of legal measures for protection of the woman and to avoid that the offence remains unpunished. The issue of the report of injuries causes sometimes worrying for the healthcare professionals about eventual negative effects deriving from such action, especially in those cases when the woman stated that she does not agree with it. Those effects might be related with the rejection and loss of trust by the woman because her wishes have not been respected, with the possibility of rupture of the relationship healthcare professional-patient, and the eventual increase of risk for the health or life of the woman because of reprisal from the aggressor. Having in mind that each case is a particular one and that an individual analysis and assessment of the situation that each woman is in, must be made, it is recommended to conduct the action that have been explained in the concerned chapters.

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
44
ACTION TOWARDS THE ILL-TREATER
The competence for intervention and treatment of ill-treaters for their eventual recovery and reintegration concern the Ministry of the Interior and the institutions and organizations concerned and linked to the same. With regard to the ill-treater, the only competences of sanitary action are those related with the need of assistance, as a user, derived from his state of health. In those cases when he, himself –as a patient– asks for help from the sanitary services in order to change his violent behaviour, he would be offered information about the available resources in his autonomous community for cases like his. In case that the ill-treated woman asks from the healthcare staff help for her intimate partner or former intimate partner, the action would be as in the above case, offering information about the concerned available resources in the range of her autonomous community.

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
45
REPORT OF INJURIES AND MEDICAL REPORT
The Organic Law 1/2004 of December 28th, about Measures for Integral Protection against Gender-Based Violence, in its Title III establishes, about Institutional Tutelary, in its Article 32, concerning Cooperation Plans, that:
«The protocols, further to their reference about the procedure to be conducted, will make express reference to the relationship with the Administration of Justice, in those cases when there is ascertainment or well-founded suspicion of physical or psychical damaged caused by these aggressions or abuses».
On the other hand, the article 262 of the Code of Criminal Procedure states that:
«Those who because of their posts, professions or craft had known about any public offence, are compelled to immediately report it to the Prosecutor, the competent Court, the Magistrates Court or, in want of it, to the constable or police officer that were closest to the place, if it is an actual crime».
The obligation is considered fulfilled by sending the report of injuries. According to what the Code of Criminal Procedure states, the Prosecutor may, previously to legal action – before the corresponding report of the offence reached the concerned Judge and before he issues his verdict – order the issue of preliminary proceedings, in order to obtain more data and information about the reported facts. Sending the report of injuries, in general, to the judicial authority means its entry registration and remittance to the Deanery of the Courts*. Once the entry registration of the report of injuries in the concerned judicial office has taken place, the procedure of the trial will be the same as if the report was issued by the woman or people close to the same (neighbourship, friendship).
* Deanery: Organization, within the office of the concerned judicial district, which is in charge, among other things, of assigning matters among the different courts attached to it.

46
Common Protocol for Healthcare Action against Gende r-Based Violence
At the Deanery it will be decided which Court will know about the case, having in mind, in the first place, the class of the competent Court, according to the legislation in force. In the second place, if in that judicial district there is more than one Court of the same class, the one that is correspondent will know of the case according to the application of assignment rules that are previously approved by the Deanery. After having received the report of injuries, the Judge will command the commencement of the penal proceedings (or he will include it with the penal procedure already commenced, if he has already about the facts) and will decide conducting preparatory inquiries, and in its case, the adoption of protection measures for the victim. It is very important to identify the cases of gender-based violence as such, so that at the Deanery they know that the procedure must be handled at a competent court for gender-based violence matters, and so accordingly remitted. Otherwise, it might be sent to a Magistrates Court without those competences that would have it inhibit itself once they discovered it was a case of gender-based violence, what would delay processing with prejudice for the woman. The report of injuries and the clinical report will have to be made by the doctor responsible of the assistance, following the recommendations given below, and with compulsory remittance to the Magistrates Court. It must be filled out with clear, legible letters and without blotting out (it may be interpreted as a manipulation). It is recommendable to computerize the report of injuries and the medical report, since that would avoid the problems with illegible letters, wrong fulfilment, empty boxes, etc. Sometimes, the illegibility of the reports prevents from knowing the exact magnitude of the injuries, of the complementary examinations and other data of interest, and consequently the seriousness of the aggression. That makes more difficult the later expert assessment by the forensic surgeon, and consequently also the assessment by the Judge. Concerning the report of injuries and the adjoined medical report, following there are some guide-lines about the data that is convenient to fill out regardless of the blank that each Autonomous Community may have established in its territory. The report of injuries and the medical report will be available in all the healthcare centres. One exemplar will be delivered:

47
Common Protocol for Healthcare Action against Gende r-Based Violence
To the concerned person provided it does not endanger her safety (she may have come accompanied by the alleged aggressor or it may be that when arriving home, the aggressor may discover the copy). In this case, if she is afraid to take the copy with her, she may be suggested, it can be handed to some relative or a person whom she can trust. To the court, by mail. In those cases when there is urgency for the notification, it will be sent via fax. It will be filed along with the clinical report of the woman in the sanitary centre where she was assisted.
It is important to relieve that: The medical report must be read to the woman before its end issue

48
Common Protocol for Healthcare Action against Gende r-Based Violence
REPORT OF INJURIES AND MEDICAL REPORT *
DATA OF THE HEALTHCARE STAFF, RESPONSIBLE FOR THE ASSISTANCE :
Hospital / Healthcare Centre / Consultation
Data of the professional that issues it: First name and Family names, CNP
DADES DE FILIACIÓ DE LA VÍCTIMA :
First name and family names IDENTIFICATION CARD or IDENTIFICATION NUMBER FOR IMMIGRANTS Date of birth, Age Country of origin Marital Status Address, Municipality (Post Code or INE Code) Telephone
INJURIES PRESUMABLY PRODUCED BY THE AGGRESSION, AND THEIR TYPE
Type of exerted violence
Use of objects for the aggression
Psychical and emotional condition. (Describe the emotional symptoms and the attitude of the woman). Psychological ill-treatment can be reflected in symptoms of depression, anxiety, suicidal trends, somatology, posttraumatical stress syndrome). The emotional condition of any person with an injury is disturbed , but the attitude varies. This can be a great indicator of what has happened, for example: an ill-treated woman may feel herself perplexed, fleeing, reckless, frightful, aggressive, hyperalert, apathetic, inexpressive… This information is necessary in order to approach the psychical condition of the woman.
Present Physical injuries: It is important that the injuries (cutaneous, muscle skeletal, ocular, auditive, genital, internal, etc) are described in detail concerning type, shape, size, colour and location, what will help to know their date or eventual date they took place. With that purpose, special attention will be paid to the oldest injuries or in a different state of evolution, as a proof of their habitualness or repeatedness. It is recommended to take pictures (preferably in colour) of the injured areas, with previous consent of the woman.
* Even when the report of injuries and the medical re port may have different formats and supports, it is necessary that they inc lude at least this information .

49
Common Protocol for Healthcare Action against Gende r-Based Violence
When there is the possibility of any internal injury, after their clinical assessment (abdominal, thoracic and / or cervical), this information will be collected only in quality of suspicion, since only after making the diagnostic tests, at hospital level, they will be confirmed.
Other CLINICAL data
Complementary conducted tests
Theurapeutical measures (include prophylactic measures, pharmacological treatment, local cures, surgical treatment, etc.)
Clinical prognosis
DATA CONNECTED WITH THE FACTS THAT PROMPTED THE ASSISTANCE
In this section it will be reflected how the facts happened, by using, and writing between quotation marks, whenever possible, the same works of the woman. Furthermore it will include:
Address, place of the aggression , date and time of the incident Date / time of the assistance Origin of the injuries as stated by the woman: Physical, psychical, sexual Suspicion that the cause of the injuries is a different one from that stated by the woman
ANTECEDENTS
She turns on alone or accompanied by (name and kindred/ relationship) One-time aggression, the first time or repeated ill-treatment In case that the aggression are being suffered since some time ago, state since when and described the characteristics of these aggressions, their type, frequently (daily, weekly, monthly…), if the intensity of violence is growing, if any report has been previously made, etc, and their evolution. Other people that have suffered ill-treatment during the same incident or in other occasion (if the woman has minors or other dependant people in charge of her and that are also victims of ill-treatment, this has to be notified to paediatrics and social work of the centre. If it is deemed convenient, to the concerning Service for Protection to Minors) Witnesses: Acquaintances (neighbourhood, friends), minors or other dependent people in charge of her.

50
Common Protocol for Healthcare Action against Gende r-Based Violence
DATA OF THE ALLEGED AGGRESSOR :
First name and family names
Relationship / kindred with her aggressor
Address or supposed telephone
PLAN OF ACTION
According to the case, include the discharge report or derivation to other specialties and resources, ingress in hospital if it has been necessary, and the required follow-up.
OTHER DATA
Connected with those situations that are not collected in the previous sections and that need to be stated to the Court, such as, for example:
If it has been informed to the Court on the telephone, and if it has been done, specify when
Safety aspects and danger perceived by the woman
Attitude of the woman towards presenting a report
REMARKS
In this section will be included those data that have not been previously described, but that are deemed convenient. Even when the offences concerning ill-treatment are public offences that will be prosecuted ex-officio, in this section it must be stated if the woman has manifested that she does not want to make a report and the cause of it (fear from the aggressor, fear to lose the custody of her children, to the reaction of her family, economical dependence, etc), in order to offer the judicial agency information about the circumstances the woman is in, that might help approaching this specific case. In case that there is evidence of previous injuries that might direct towards the conviction or founded suspicion that the woman is suffering habitual ill-treatment, it is important to reflect it in the report of injuries, because this is another different offence from just injuries . The existence of other threatening by the aggressor (verbal, announcing that he is going to use another instrument for aggression, etc) will also be stated It is convenient to have several EXEMPLARS: for the concerned person / the Court/ Sanitary Centre (and / or clinical report) and / or Central Sanitary Register

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
51
GLOSSARY OF TERMS
Algorithm for action: finite and organized assembly of actions, that can be presented graphically, facing a problem or a certain circumstance. Screening: epidemical program intended for detection in a certain and asymptomatic population, a serious health problem in its initial or early stage, with the purpose of diminishing the associated morbidity-death rate by means of an effective or curing intervention. There are universal screening programs that are applied systematically to the whole of the population and selective screening programs. In order that the former are applied, certain pre-existent conditions must exist, among them the availability of an effective and accepted by the population treatment, in case that the disease has been found in its initial stage and that the screening test has given a good cost-effectiveness relationship (in the cost is included the economical one, but also the increase of risks, the impact on the will-being of the person, etc). If these conditions are not present, among others, screening of the population or universal is not recommended, and in any case selective screening programs will be applied, only addressed to a population that is thought to be more prone to suffer from the disease or problem. Early detection: Identification in a certain and asymptomatic population, of a serious health problem in its initial or early stage, with the object of diminishing the associated morbidity-death rate by means of an effective and curing intervention.
Gender: gender concerns the different roles, rights and responsibilities that have been traditionally and through the socialization process assigned to men and women, as also the inequalities that it generates between them. Medical report: It consists in the description and assessment in writing, that the healthcare staff make of the injuries found. Ill-treatment: any action, emission or negligent treatment that infringe the basic rights of the person and endanger the accomplishment of the basic needs of the person and prevents or interfere the physical, psychical and / or social development. It also includes physical, psychical and sexual ill-treatment against minors, elderly people or dependent people (those that because of lack

52
Common Protocol for Healthcare Action against Gende r-Based Violence
or loss of physical and / or psychical capacity are in a situation of dependence from others). In case of ill-treatment against minors the notification to the Court will have to be issued and transacted according to the proceedings established in each Autonomous Community.
Report of injuries: medical-legal document with compulsory notification to the competent Court, concerning any injury that might be a cause of misdemeanour or offence. It is the starting point of preliminary proceedings or penal summary because of injuries or death.
Primary prevention: a set of sanitary actions carried out by the community or the governments and also by the healthcare staff before a certain health problem appears. It includes promoting health, health protection and chemical prophylaxis or vaccination.
Secondary prevention: (see screening, early detection).
Third prevention: restoring health once the disease has appeared. It is the application of an intervention to try to cure or palliate a health problem or certain symptoms.
Secondary victimization: it concerns the fact that the ill-treated woman, in addition to being the victim of the ill-treatment situation, sometimes is also blamed for this situation.
Gender-based violence: Every violent action based to the appurtenance to the female sex, that has as a result or may have some physical, sexual or psychological harm or suffering, as also threatening about such actions, coactions or deprivation of liberty, so much if they are produced in the public life, as in the private one. Gender-based violence is produced as a consequence of the unequal relationship between men and women and the existence of the «culture of violence» as the means to solve conflicts.

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
53
BIBLIOGRAPH Y
• Aguar-Fernández M, Delgado-Sánchez A, Castellano-Arroyo M, Luna del Castilo JD. Prevalence of ill-treatment in women that consult their family doctor. Primary Attention 2006; 37:241-2.
• Alberdi I, Matas N. Domestic violence. Report about ill-treatment to women
in Spain. Fundación La Caixa.2000
• Alonso M, Bedoya JM, Cayuela A, Dorado M, Gómez M, Hidalgo D. Violence against the woman. Results of a hospital inquiry. Progress in Obstetrics and Gynaecology 2004; 47:511-20.
• General Assembly of the United Nations. Declaration about the elimination
of violence against the woman. December 1993. A/RES/48/104. 23 of February 1994 [Accessed on the 21st January 2007]. Available at: http://www.acnur.org/biblioteca/pdf/1286.pdf
• Blanco Prieto P, Ruiz-Jarabo C, publishers. Prevention and detection of
violence against women by the primary healthcare. Madrid. Association for the Defence of Public Health, 2002
• (BOE) Official State Gazette of the 16th. September 2006. Royal Decree
1030/2006, of the 15th September, by which the portfolio of common services of the National Healthcare System and the procedure for its updating is established. Ministry of Healthcare and Consumption. [Accessed on the 21st. January 2007]. Available at: http://www.boe.es/boe/dias/2006/09/16/pdfs/A32650-32679.pdf
• (BOE) Official State Gazette of the 28th December 2004. General
Resolutions. Central state office. Organic Law 1/2004, of the 28th December, concerning integral protection measures against gender-based violence. [Accessed on the 10th March 2006]. Available at: http://www.boe.es/boe/dias/2004/12/29/pdfs/A42166-42197.pdf
• Reina Sofía Center for the study of violence. Statistics for femicide
[accessed the 9th February 2006] Available FT at: http://www.gva.es/violencia/
• Claudia García-Moreno. Violence against the woman: gender and equity on the health Washington, D.C.: OPS, 2000

54
Common Protocol for Healthcare Action against Gende r-Based Violence
• International Council of the National Healthcare System. Sanitary protocol for domestic ill-treatment: plan of action against domestic violence (1998-2000). Madrid: Ministry of Labour and Social Affairs and Institute for the Woman; 2000
• Delgado A, Aguar M, Castellano M, Luna del Castillo JD. Assessment of a scale
for measuring ill-treatment against women. Primary Attention, 2006, 38 (2): 82-9. • E-leusis. Monthly epidemical Index. Death rate through violence from the intimate
partner in Spain [consulted on the 22nd January 2006]. Available at: http://www.e-leusis.net/Alerta_Violencia.htm Q5
• Federation of Separated and Divorced Women. Document finder about Violence
against Women [accessed on the 22nd January 2006]. Available at: http://www.separadasydivorciadas.org/
• Fernández Alonso MC, Herrero Velázquez S, Buitrago Ramírez F, Ciurana Misol
R, Chocrón Bentata L, García Campayo J, et al. Violencia Doméstica. SEMFYC. Madrid; 2003.
• Fernández Alonso, M.C., Herrero Velázquez, S., Buitrago Ramírez, F. Ciurana
Misol, R., Chocron Bentata, L., García Campayo, J., Monton Franco, C., Redondo Granado, M.J., Tizon García, M.J. (2003). Violence within the intimate partner: role of the family doctor. Primary Attention, 32, 425-33
• García-Moreno C. Dilemmas and opportunities for an appropriate health-service
response to violence against women. Lancet 2002; 359:1509-1514. • García-Moreno C. International conference on “the role of health professionals in
addressing violence against women”: an overview. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 2002; 78(Suppl. 1): S1-S4.
• Gill-González D, Vives-Cases C, Álvarez-Dardet C, Latour-Pérez J. Alcohol and
intimate partner violence: do we have enough information to act? Eur J Public Health 2006; 16:278-84.
• Golding JM. Intimate Partner Violence as a Risk Factor for Mental Disorders: A
Meta-Analysis. J Fam Violence 1999; 14:99-132. • Heise L, Ellsberg M, Gottemoeller M. Ending violence against women. Population
Reports, Series L, nº11. Baltimore: Johns Hopkins University School of Public Health, Population Information Program; December 1999
55555555
Common Protocol for Healthcare Action against Gende r-Based Violence
• Jiménez Cassado C, Lorente Acosta M. Violence against Women, sanitary scope. Sevilla; Andalusian Institute for the Woman; 1999
• Krantz G, García-Moreno C. Violence against women J Epidemiol Community Health. 2005 Oct;59(10): 818-21
• Krantz G. Violence against women: a global public heath issue! J Epidemiol Community Health 2002; 56:242-243.
• Krug E, Dahlberg L, Mercy J, Zwi A, Lozano R, eds. World report about violence and Health. Geneva: World Health Organization; 2002/[Accessed 21st January 2007]. Available at: http://www.paho.org/Spanish/DD/ PUB/Violencia_2003.htm
• Larrión Zugasti JL, de Paúl Ochotorena J. Mujer, violence and health. Med Clin (Barc) 2000; 115:620-24.
• Matud Aznar P. Impact of domestic violence on the health of the ill-treated woman. Psicothema, 2004; 16:397-401.
• Ministry of Labour and Social Affairs and Institute for the Woman. Statistics. Women in figures. Violence. [Accessed on the 20th January 2007]. Available at: http://www.mtas.es/mujer/mujeres/cifras/violencia/index.htm#violencia
• Ministry of the Interior: Statistical Yearbooks [accessed on the 22nd January 2006] Available FT at: //www.mir.es/sites/mir/otros/publicaciones/catalogo/ unidad/ secgenTecnica/periodicas.html
• Nogueiras García B et al (Publishers). Sociosanitary attention for violence against women. Madrid. Institute for the Woman; 2004.
• United Nations Organization. IV World Conference about the Woman. 1995. [Accessed on the 21thJanuary 2007]. Available at: http://www.onu.org/ documentos/confmujer.htm
• World Health Organization, Violence against women. A priority health issue. OMS/OPS; 1998.
• Plazaola Castaño J, Ruiz Pérez I, Escribá Agüir V, Jiménez Martín JM. Spanish adaptation of a diagnosis instrument and another for screening, to detect violence against woman in the intimate partner from the sanitary scope. OSM, 2006. Available at: http://www.msc.es/organizacion/sns/ planCalidadSNS/pdf/equidad/genero_vg_01.pdf

56565656
Common Protocol for Healthcare Action against Gende r-Based Violence
• Plazaola-Castaño J, Ruiz Perez I. Intimate partner violence against women and physical and mental health consequences. Med Clin (Barc). 2004;122:461-7.
• Ramsay J, Richardson J, Carter YH, Davidson LL, Feder G. Should health
professionals screen women for domestic violence? Systematic review. BMJ 2002; 325(7359):314.
• Report about the victims of gender-based violence, year 2006.
http://www.separadasydivorciadas.org/muertas2006.html • Romito P, Molzan TJ, De Marchi M. The impact of current and past interpersonal
violence on women´s mental health. Soc Sci Me 2005;60:1717-27. • Ruiz Pérez I, Plazaola Castaño J. Intimate Partner Violence and Mental Health
Consequences in Women Attending Family Practice in Spain. Psychosom Med. 2005;67:791.7.
• Ruiz-Perez I, Blanco-Prieto P, Vives-Cases C. Violence against woman in the
couple: determinants and sociosanitary answers. Gac Sanit. 2004; 18 Supl 2:4-12.
• Ruiz-Perez I; Jiménez Rodrigo ML; Bermúdez Tamayo C, Plazaola Castaño J.
Catalogue of Instruments for Screening and Frequency of physical, psychological and sexual ill-treatment, OSM, 2006. Available at: http://www.msc.es /organizacion/sns/planCalidadSNS/pdf/equidad/genero_vg_01.pdf
• Siendones Castillo R, Perea-Milla E, Arjona JL, Aguera C, Rubio A, Molina M. Domestic violence and healthcare professionals: knowledge, opinions and barriers for the infradetection. Emergencies 2002;14:224-232.
• U.S.Preventive Services Task Force. Screening for family and intimate partner
violence: Recommendation statement. Ann Fam Med 2004; 2:156-160. • Walker L. The battered woman syndrome. Springer, New York; 1984. • Wathen CN, MacMillan HL. Interventions for Violence Against Women: Scientific
Review. JAMA 2003; 289(5):589-600. • WHO Multi-Country Study. On Women´s Health And Life Events. Department of
Gender and Women´s Health. Family and Community Health. World Health Organization. Geneva 2003.
• World Health Organization (WHO). Multi-country Study on Women´s Health and Domestic Violence against Women. Geneva: WHO; 2003.

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
57575757
ANNEX PROTOCOLS AND
GUIDE-LINES FOR HEALTHCARE ACTION
OF THE AUTONOMOUS COMMUNITIES
Andalusia Sanitary attention to women victims of ill-treatment. Strategic Plan, Andalusian Healthcare Service. Health Council-House. Cabinet Board of Andalusia. (2001) Report of injuries and medical report for supposed cases of domestic violence, ill-treatment against minors and elderly people and sexual aggressions. Cabinet of Andalusia. (pending publication). Aragon Guide-lines for sanitary attention to the woman victim of domestic violence, in the healthcare system of Aragón. Government of Aragón. Department of Health and Consumption. General Administration for Planning and Securing (2005) Asturias Protocol for sanitary attention for violence against women. Healthcare Service of the Principality of Asturias. Government of the Principality of Asturias (2003) Balearics Strategies for prevention and treatment of domestic violence. Council for Social Well-being. Institute for the Woman. Balearic Government.(2002)

58585858
Common Protocol for Healthcare Action against Gende r-Based Violence
Canarias Instruction 3/03 by means of which the official document blanks and paperwork to be filled out by the healthcare staff in cases of sanitary assistance for injuries that might constitute a misdemeanour or offence. Council-house of Healthcare and Consumption. Canarian Healthcare Service. Gender-Based Violence and Health: Handbook and Didactical Units for sensitization and prevention. Government of Canarias. Coedition of the Council-house for Healthcare and Consumption. Canarian Healthcare Service and Canarian Institute for the Woman (2005) Protocol of Action against gender-based violence in the domestic scope. Government of Canarias. Council-House of Healthcare and Consumption. Canarian Healthcare Service (2003) Cantabria Protocol of Sanitary action against ill-treatment. Government of Cantabria. Council-House for Healthcare and Social Services. General Administration for Public Health (2006) Violence against women Protocol of sanitary action against ill-treatment, Government of Cantabria. Council-House for Healthcare and Social Services. General Administration for Public Health (2005) Castilla y León Guide-lines for action against ill-treatment against the Woman. Castilian and León Society for Family and Community Medicine (SocalemFYC) (2005) Net of Assistance to the woman suffering ill-treatment. Council-House for Healthcare and Social Well-being. Government Board of Castilla and León .(2003) Castilla-La Mancha Protocol for Primary Attention Action for women victims of ill-treatment. Council-House for Healthcare. General Administration for Public Health and Participation. Castilla-La Mancha. (2005)

59595959
Common Protocol for Healthcare Action against Gende r-Based Violence Cataluña Guide-lines for approaching gender-based ill-treatment in the Primary Attention. Catalan Institute for Healthcare Department of Healthcare and Social Security. Generalitat de Catalunya. (2003) Protocol and circuit for approaching gender-based violence in the scope of healthcare in Catalunya. Healthcare Department. Generalitat de Catalunya. ( Document under elaboration phase) Recommendations for sanitary attention of ill-treated women. Collection: Healthcare Plan. Issue number 14. Catalan Healthcare Service. Department of Healthcare and Social Security. Generalitat de Catalunya (2004) Comunidad Valenciana Medical Report for Alleged Domestic Violence (adults). Generalitat Valenciana. Council-House for Healthcare (2005) Extremadura Interdepartmental Protocol for eradication and prevention of violence against the woman. Institute of Extremadura for the woman. Government Board of Extremadura (2001). ANNEX 1. Guide-lines for action by professionals concerned in the emergency itinerary. Galicia Approach to gender-based violence from the sanitary scope. Guide-lines for prevention, detection and attention in gender-based violence in the sanitary area. Xunta de Galicia (2002) Defend your rights. Practical guide-lines for women suffering gender-based violence. Xunta de Galicia (2007) Guide-lines for Gender-Based Violence in the Healthcare Primary Attention. Xunta de Galicia (2005)

60606060
Common Protocol for Healthcare Action against Gende r-Based Violence
Madrid Violence against women considered as a public Health problem. Document of Support for the healthcare attention of the victim women. Institute for Public Health. Community of Madrid (2003) Murcia Protocol for Coordination of the Force and Security State Corps with the Judicial Organs, Professional Colleges and others concerned in the protection of violence victims from Gender-Based Violence. Region of Murcia. (2000) Navarra Protocol for coordinated action for assistance to victims of gender-based violence. Guide-lines for professionals. Department for Social Well-being. Sports and Youth. Institute of Navarra for the Woman. Government of Navarra. (2006) País Vasco Healthcare Protocol for domestic ill-treatment. Department for Healthcare. Basque Government (2000) included in the frame of the Interinstitutional Agreement for the improvement of the attention to women victims of domestic ill-treatment and sexual aggressions (2001). (The healthcare protocol is now in process of revision/updating) La Rioja Integral Program for Detection and Approach for Domestic Violence, from the Public Healthcare System of La Rioja. Riojan Healthcare Service. (2004)

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
61616161
NOTES

62626262
Common Protocol for Healthcare Action against Gende r-Based Violence

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género

Protocolo Común para la Actuación Sanitaria ante la Violencia de Género
MINISTRY
FOR HEALTHCARE
AND CONSUMPTION