nuestra experiencia en las terapias libres de ifn y rbv en … aoufi, terapias libres de ifn...
TRANSCRIPT

NUESTRA EXPERIENCIA
EN LAS TERAPIAS
LIBRES DE IFN Y RBV EN
PACIENTES RENALES
CON VHC
SAMI AOUFI RABIH
UNIDAD HEPATORRENAL, SERVICIO DE APARATO DIGESTIVO
HOSPITAL LA MANCHA-CENTRO

GENOTIPOS VHC
RVS
< 50%
RVS
> 80%

Adaptado de Davies et al, Liver Transplant 2003

MANIFESTACIONES
EXTRAHEPÁTICAS VHC
Glomerulonefritis
Reumatológicas
Oftalmológicas
Dermatológicas
Neurológicas
Hematológicas

GN-VHC
TIPOS
• Membranoproliferativa
• Membranosa
• Ig A
• Otras
CLÍNICA
• Proteinuria ±
microhematuria ± IR
• Remisión espontánea
infrecuente
FACTORES DE PROGRESIÓN A
CIRROSIS

POBLACIÓN RENAL
Polifarmacia Comorbilidad Inmunosupresión Riesgo de
transmisión nosocomial
Transaminasas normales
Carga viral baja Evolución de la
hepatopatía
Efecto antiviral sobre la función
renal
Candidatos a trasplante renal

Coagulopatía
• Insuficiencia hepática • Trombocitopenia por HTP • Disfunción plaquetaria • Anticoagulación intradiálisis • Antiagregación
Ascitis
Punción de la cápsula de Glisson
GPVH
Evaluación de la fibrosis y la actividad necroinflamatoria (METAVIR)
Exclusión de causas concomitantes de daño hepático (hemosiderosis,
HGNA, etc.)
BIOPSIA HEPÁTICA


CORRELACIÓN CLÍNICA,
ANALÍTICA Y RADIOLÓGICA
García Agudo R et al, Nefrología 2011;31(4):489-504

DATOS EPIDEMIOLÓGICOS DE LA
HEPATITIS C EN PACIENTES RENALES

Población general 3% OMS
Hemodiálisis 13% (1-70%) Aoufi et al, Nefrología 2011
Hemodiálisis España
2010-2011
5,6% Aoufi et al, Nefrología 2013
Trasplante renal 7-40% Pereira et al, Kidney Int 1998
Hanafusa et al, Transplantation 1998
Vosnides, Kidney Int 1997
García Agudo R et al, Nefrología 2013;33(2):188-95
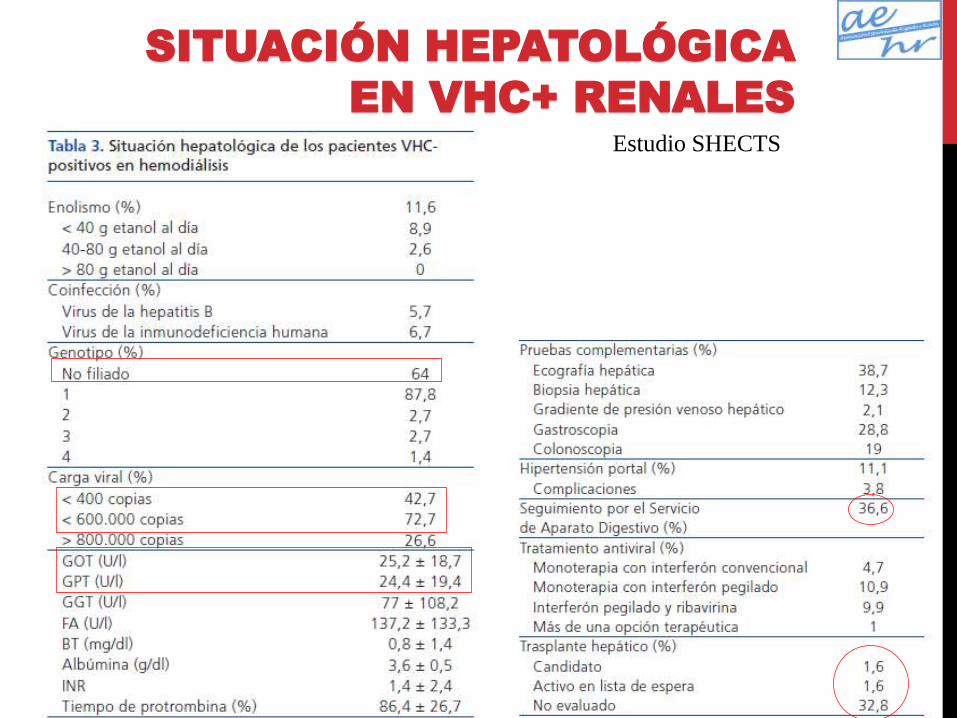
Estudio SHECTS
SITUACIÓN HEPATOLÓGICA
EN VHC+ RENALES

10,8
2,1
73,7
18,6
28,4
38,7% digestiva
0 10 20 30 40 50 60 70 80 90 100
Biopsia hepática
Hemodinámica
Ecografía
Colonoscopia
Gastroscopia
F0 – 23,8%
F1 – 23,8%
F2 – 28,5%
F3 – 4,7%
F4 – 4,7%
No filiado – 14,5%
SITUACIÓN HEPATOLÓGICA EN VHC+ RENALES

Estudio SHECTS
0
10
20
30
40
50
60
70
80
90
100
No tratamiento IFN convencional IFN peg IFN peg + RBV Varios
73,4
4,7
10,9 9,9
1
Tratamiento del VHC
SITUACIÓN HEPATOLÓGICA EN
VHC+ RENALES
García Agudo R et al, Nefrología 2013;33(2):188-95

Hipertransaminasemias tratadas (%)
Pacientes tratados seguidos en Digestivo (%)
28
51,4
Glomerulonefritis tratadas (%)
Candidatos a trasplante tratados (%)
36,1
51,4
Duración del tratamiento (meses)
Respuesta viral sostenida (%)
7,4 ± 5
44,4%
Suspensión del tratamiento (%)
Ausencia de respuesta
Anemia
Intolerancia
Psicosis
Otros
67,4
35
31
21
3
10
Estudio SHECTS
SITUACIÓN HEPATOLÓGICA EN
VHC+ RENALES
García Agudo R et al, Nefrología 2013;33(2):188-95

García Agudo R et al, Nefrología 2013;33(2):188-95
ETIOLOGÍA IRC EN VHC+
RENALES
Estudio SHECTS

MANEJO CLÍNICO ÓPTIMO DEL PACIENTE
RENAL

VHC + TR
1ª causa de disfunción hepática post-TR
4ª causa de mortalidad en TR
Reactivación del VHC en TR
Evolución acelerada a cirrosis y CHC
hepatitis colestásica fibrosante
Factor independiente para proteinuria
Diabetes post-TR
Glomerulonefritis de novo
Nefropatía crónica del injerto
Infecciones
supervivencia en HD y TR
supervivencia del injerto
Benhamou Y et al. Hepatology 1999;30(4):1054-8
Pereira BJ et al. Kidney Int 1998;53(5):1374-81
Hanafusa T et al. Transplantation 1998;66(4):471-6
Vosnides GG. Kidney Int 1997;52(3):843-61
Martin P et al. Transplantation 2000;69(7):1479-84
Cotler SJ et al. J Clin Gastroenterol 2002;35(2):191-5

Sujetos VHC+ no tratados con cirrosis compensada
Sujetos VHC+ no tratados con ERC y cirrosis compensada
91% a los 5 años
76% a los 5 años
Keith DS et al, Arch Intern Med 2004;164:659–663
SUPERVIVENCIA VHC+ RENALES


EVOLUCIÓN DEL
TRATAMIENTO Y LA RVS
0 20 40 60 80 100
1991
1995
1998
2001
2001
2012
2014
IFN (6 meses)
IFN (12-18 meses)
IFN / RBV (6-12 meses)
IFN peg (6-12 meses)
IFN peg / RBV (6-12 meses)
IFN peg / RBV / IP1
IP2 ???

Pyenson, Milliman Report 2009
INCIDENCIA VHC
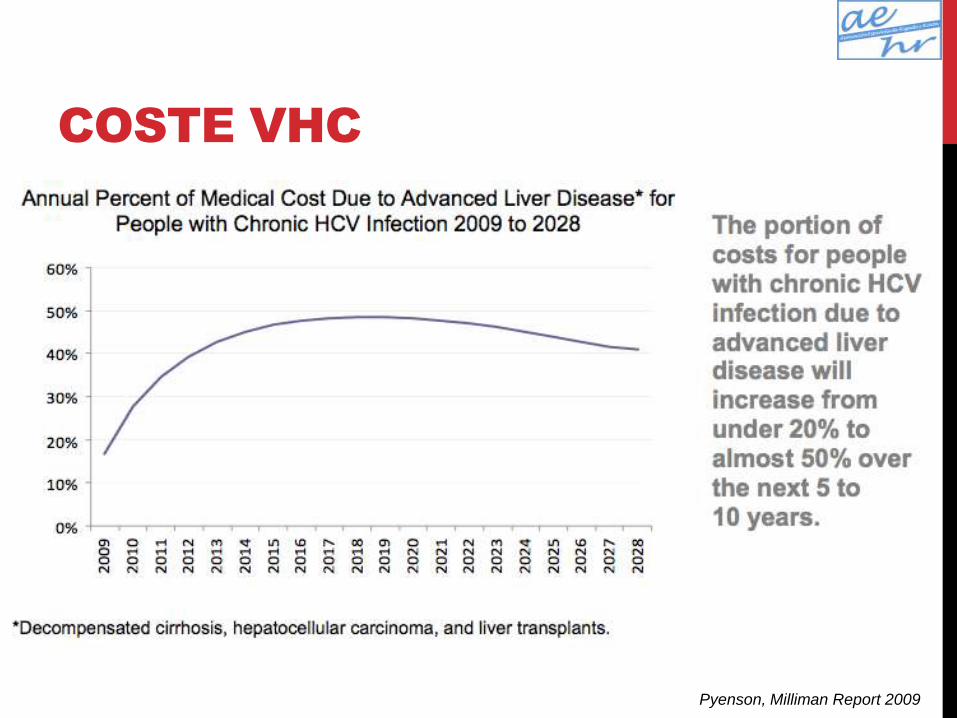
Pyenson, Milliman Report 2009
COSTE VHC

PRESENTE



TTO VHC+ RENALES: PAUTA
Dosis reducidas de IFN peg en monoterapia ± RBV en FGe > 50 ml/min
IFN + ribavirina (200 mg x 3
veces/sem) en diálisis
Poca experiencia
Series de casos,
bajo nº pacientes
Mejor RVS
Hepatology 2005;42(Suppl):703-4
J Viral Hepat 2006;13(5):316-21
Nephrol Dial Transplant 2008;23(2):721-5
Clin Pharmacol Ther 2000;68(5)556-67
Int J Artif Organs 2008;31(4):295-302
Semin Liver Dis 1999;19(Suppl 1):17-24
Nephron 1998;80(1):51-6
J Am Soc Nephrol 1998;9(12):2344-8

AUTORES Nº G1 TRATAMIENTO RVS SUSPENSIÓ
N
Bruchfeld et al (J Viral Hepat, 2006) 6 84% IFN x 3 veces/sem + RBV 170-300 mg/24 h 16% (1/6) 33%
Bruchfeld et al 6 67% IFNp-2b 50 mcg/sem / IFNp-2ª 135 mcg/sem + RBV 170-
300 mg/24 h
50% (3/6) 33%
Tseng et al (AJKD, 2013) 26
26
IFNp-2b + RBV vs IFNp-2b 62% vs 27% 15% vs 23%
Hakim et al (Digestive Disease Week, 2006) 20 90% IFNp-2a 135 mcg/sem + RBV 200 mg x 3 veces/sem 5% (1/20) 67%
Mousa et al (AASLD, 2006) 20 37% IFN x 3 veces/sem + RBV 200 mg x 3 veces/sem 0,6 (12/20) 0%
Van Leusen et al (NDT, 2008) 7 57% IFNp-2a 135 mcg/sem + RBV 130-200 mg/24 h 71% (5/7) 0%
Carriero et al (Int J Artif Organs, 2008) 14 80% IFNp-2a 135 mcg/sem + RBV 200 mg/24 h 28% (4/14) 71%
Rendina et al 35 46% IFNp-2a 135 mcg/sem + RBV 200 mg/24 h 97% (34/35) 11%
Al-Saran et al 10 10% IFNp-2a 135 mcg/sem + RBV 200 mg x 3 veces/sem 70% (7/10) 0%
Alsaran et al 3 0% IFNp-2a 135 mcg/sem + RBV 200 mg x 3 veces/sem 100% (3/3) 0%
Liu et al 35 71% IFNp-2a 135 mcg/sem + RBV 200 mg/24 h 60% (21/35) 17%

AFÉRESIS
2007 2010
193 pacientes (naïve, relapsers y non-responders)
Genotipo 1b
DFPP (5 sesiones/1 sem) + tto vs no DFPP
RVR 2,47 log vs 1,52 log (p 0,01)
RVS 77,8% vs 50%
206 pacientes
181 IFNp+RBV+DFPP
RVP 57,5%
• 70% naïve
• 57,1% relapsers
• 41,9% non-responders
Fujiwara et al, Hepatol Res 2007 Kaneko et al, Hepatol Res 2010
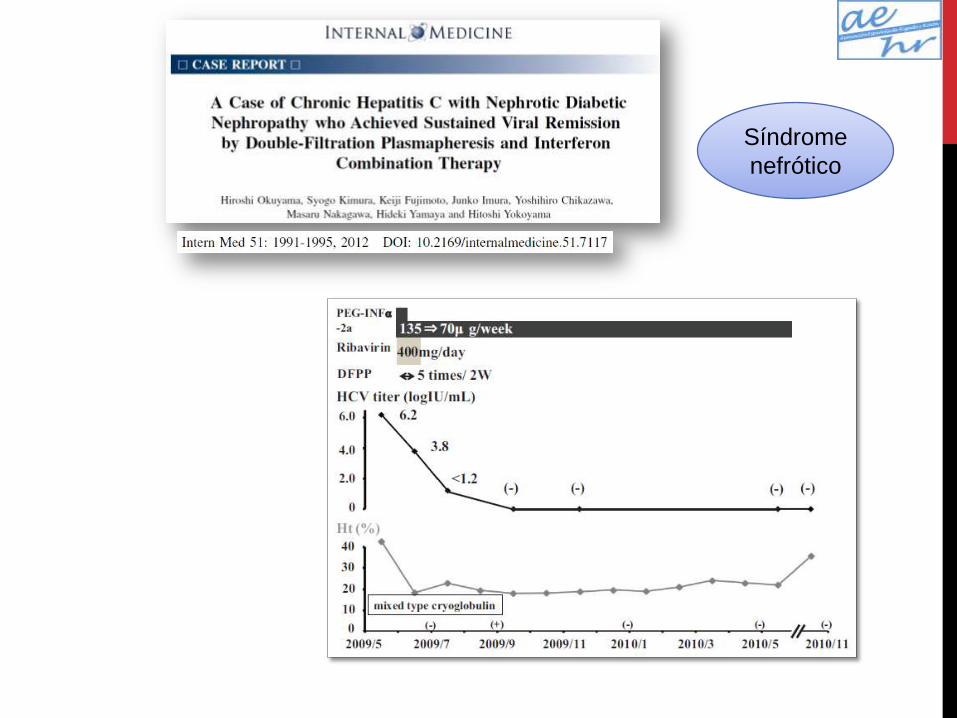
Síndrome
nefrótico

Trasplante
renal

64 años, exfumador, obesidad grado 1, HTA, glucemia basal alterada, insuficiencia venosa crónica, prótesis bilateral de cadera, herniorrafia inguinal bilateral
ERC-5D
• Riñón izquierdo atrófico
• Posible GN por VHC vs nefroangiosclerosis vs GN focal y segmentaria por obesidad
• Nefropatía tubulointersticial crónica por cólicos nefríticos de repetición
• Historia nefrológica: DP previa con suspensión por peritonitis fúngica; anemia nefrogénica, HPTS, acidosis metabólica
• Candidato a trasplante renal
Hepatopatía crónica por VHC genotipo 1b
• BHTY A3F3, GPVH 5 mm Hg
• IL-28 CT
• Tratamiento previo con IFNpeg ± RBV en otro hospital ¿? sin RVP
CASO CLÍNICO

CASO CLÍNICO
0,5-1 mcg/kg/sem 200 mcg/24-48 h 800 mg/8 h

CASO VML
5
6
7
8
9
10
11
12
13
Hemoglobina
500
1000
1500
2000
2500
3000
Neutrófilos
0
1
2
3
4
5
6
7
8
Carga viral
20000
40000
60000
80000
100000
120000
Plaquetas
↑ EPO ↓ IFN/RBV
hem
breakthrough

FUTURO

PROCESAMIENTO DE
LA POLIPROTEÍNA

COMBINACIONES DE
ANTIVIRALES
PROTEASA
Paritaprevir
(AbbVie)
Asunaprevir (Japón)
MK-5172
Simeprevir
POLIMERASA
Sofosbuvir
Dasabuvir
BMS-791325
iNS5A
Daclatasvir
Ombitavir
Ledipasvir
MK-8142

40
EFFICACY AND SAFETY OF MK-5172 + MK-8742
± RIBAVIRIN IN HCV MONO-INFECTED AND
HIV/HCV CO-INFECTED TREATMENT-NAÏVE,
NON-CIRRHOTIC PATIENTS WITH HCV GT1
INFECTION:
THE C-WORTHY STUDY
(FINAL RESULTS, PARTS A AND B)
Mark S. Sulkowski, Christophe Hezode, Jan Gerstoft, John M. Vierling, Josep Mallolas, Stanislas Pol, Marcelo Kugelmas, Abel Murillo,
Nina Weis, Ronald Nahass, Oren Shibolet, Lawrence Serfaty, Marc Bourlière, Edwin DeJesus, Eli Zuckerman, Frank Dutko, Anita Y. M.Howe, Melissa Shaughnessy, Peggy Hwang, Janice
Wahl, Michael Robertson, Eliav Barr, Barbara Haber

41
BACKGROUND
Grazoprevir (MK-5172): NS3/4A protease inhibitor
Elbasvir (MK-8742): NS5A inhibitor
Combination: high barrier to resistance
C-WORTHy Part A demonstrated an efficacy of 89-100% in
treatment naïve non-cirrhotic patients with GT1 infection
and supported expansion in Part B to more diverse
populations
C-WORTHy: Grazoprevir + Elbasvir ± RBV in 471 HCV GT1-infected
patients Treatment-naive, non-cirrhotic
12 weeks ± RBV (n = 65) Pt. A
Treatment-naive Non-cirrhotic
8-12 weeks ± RBV (n = 94) Pt.B
Treatment-naive Cirrhotic
12-18 weeks ± RBV (n = 123) Pt.B
HIV/HCV Co-infected Non-cirrhotic
12 weeks ± RBV (n = 59) Pt.B
Null Responders Cirrhotic / Non-cirrhotic
12-18 weeks ± RBV (n = 130) Pt.B
42
80 93 98 97 87
0 10 20 30 40 50 60 70 80 90
100
SVR
12
(%
)
24
30
43
44
79
85
26
30
28
29
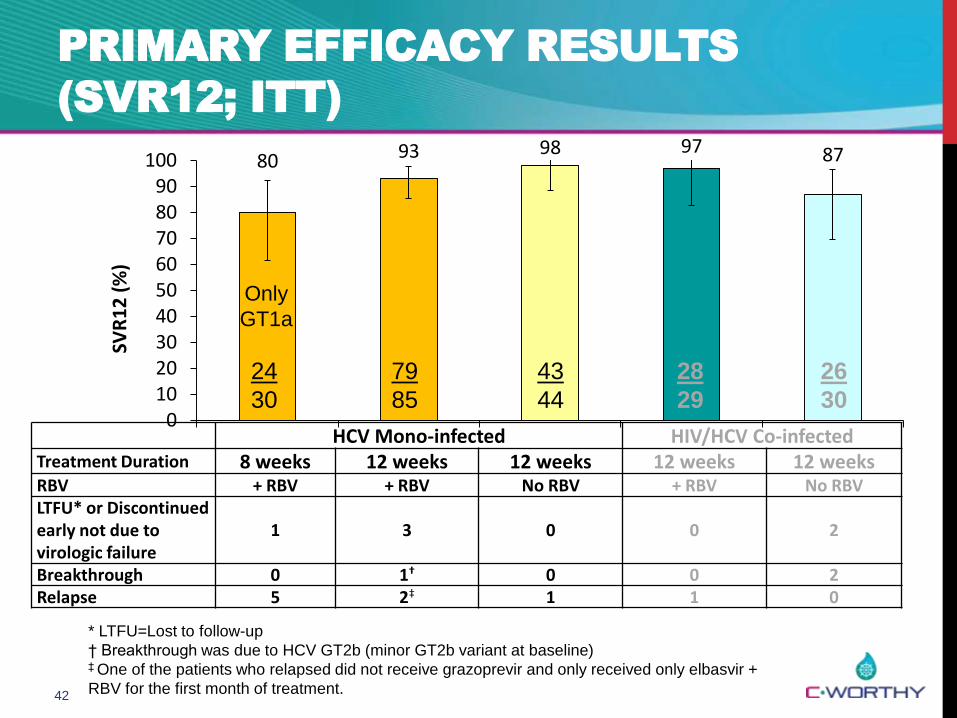
PRIMARY EFFICACY RESULTS
(SVR12; ITT)
HCV Mono-infected HIV/HCV Co-infected Treatment Duration 8 weeks 12 weeks 12 weeks 12 weeks 12 weeks RBV + RBV + RBV No RBV + RBV No RBV LTFU* or Discontinued early not due to virologic failure
1 3 0 0 2
Breakthrough 0 1† 0 0 2 Relapse 5 2‡ 1 1 0
* LTFU=Lost to follow-up
† Breakthrough was due to HCV GT2b (minor GT2b variant at baseline) ‡ One of the patients who relapsed did not receive grazoprevir and only received only elbasvir +
RBV for the first month of treatment.
Only
GT1a
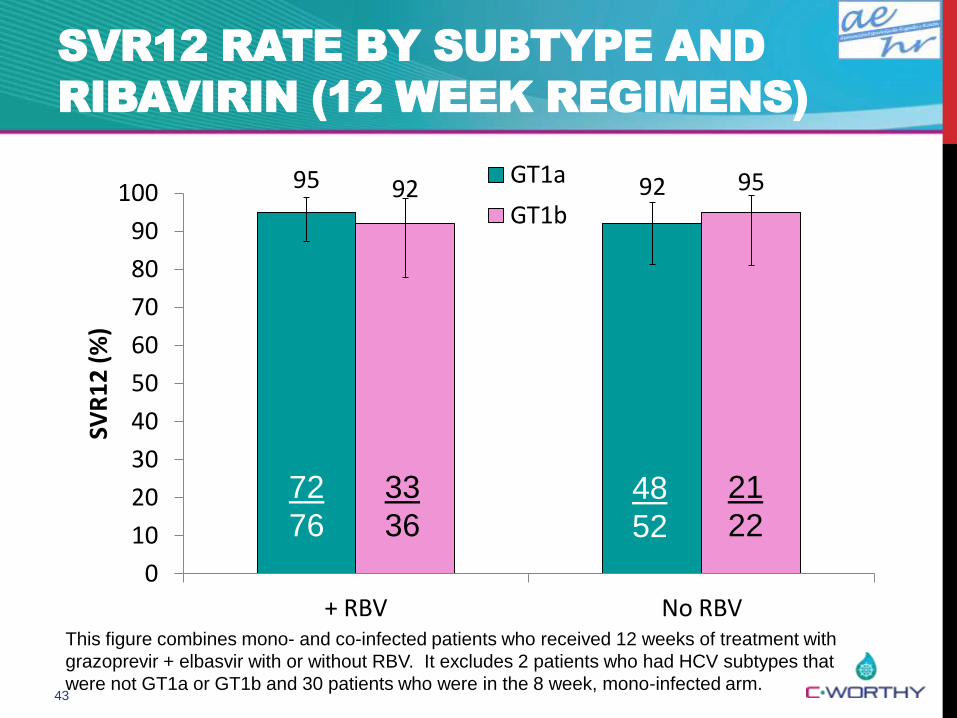
43
SVR12 RATE BY SUBTYPE AND
RIBAVIRIN (12 WEEK REGIMENS)
95 92 92 95
0
10
20
30
40
50
60
70
80
90
100
+ RBV No RBV
SVR
12
(%
)
GT1a
GT1b
72
76
33
36
48
52
21
22
This figure combines mono- and co-infected patients who received 12 weeks of treatment with
grazoprevir + elbasvir with or without RBV. It excludes 2 patients who had HCV subtypes that
were not GT1a or GT1b and 30 patients who were in the 8 week, mono-infected arm.
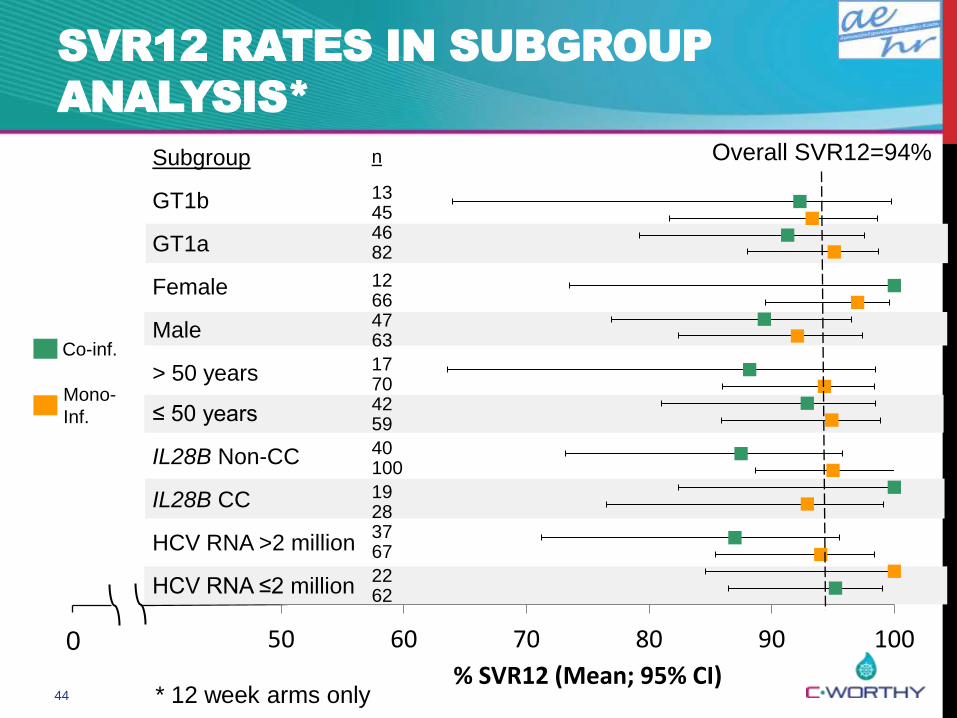
44
SVR12 RATES IN SUBGROUP
ANALYSIS*
* 12 week arms only
Co-inf.
Mono-
Inf.
Subgroup
GT1b
GT1a
Female
Male
> 50 years
≤ 50 years
IL28B Non-CC
IL28B CC
HCV RNA >2 million
HCV RNA ≤2 million
Overall SVR12=94%
0
n
13 45 46 82
12 66 47 63
17 70 42 59
40 100
19 28 37 67
22 62
50 60 70 80 90 100
% SVR12 (Mean; 95% CI)

45
HCV Mono-infected HIV/HCV Co-infected
Grazoprevir +
Elbasvir + RBV N=116*
Grazoprevir + Elbasvir (No RBV)
N=43*
Grazoprevir + Elbasvir
+ RBV N=29
Grazoprevir + Elbasvir (No RBV)
N=30
Serious adverse event 1† (1%) 0 (0%) 1‡ (3%) 1§ (3%)
Death 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Discontinued due to AE 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Hemoglobin <10 g/dL 10 (9%) 0 (0%) 1 (3%) 0 (0%)
Total bilirubin >5xULN 0 (0%) 0 (0%) 2 (7%) 0 (0%)
ALT/AST >2x to ≤5xULN after initial
normalization
1 (1%) 1 (2%) 0 (0%) 1 (3%)
ALT/AST >5xULN after initial normalization 0 (0%) 0 (0%) 0 (0%) 0 (0%)
Change in CD4 from baseline
(cells/mm3, mean (SD))
N/A N/A -47 (176) 52 (178)
HIV breakthrough N/A N/A 0 (0%) 0 (0%)
ADVERSE EVENT AND LABORATORY
SAFETY SUMMARY DURING TREATMENT
†Serious AEs were: †nausea (related to study drug); ‡ asthenia (related to study
drug); § Staphylococcal infection (not related to study drug)

46
COMMON ADVERSE EVENTS
DURING TREATMENT
HCV Mono-infected HIV/HCV Co-infected
Common Adverse Event*
Grazoprevir + Elbasvir
+ RBV N=116†
Grazoprevir + Elbasvir (No RBV)
N=43†
Grazoprevir + Elbasvir
+ RBV N=29
Grazoprevir + Elbasvir (No RBV)
N=30
Fatigue 37 (32%) 10 (23%) 2 (7%) 2 (7%)
Headache 24 (21%) 15 (35%) 4 (14%) 1 (3%)
Nausea 24 (21%) 7 (16%) 0 (0%) 1 (3%)
Diarrhea 15 (13%) 5 (12%) 1 (3%) 0 (0%)
*Incidence >10% in all arms combined;
Order in decreasing frequency based on all arms combined. † One patient received RBV but was assigned the RBV-free
arm.
For the analysis of safety, this patient is in the + RBV group.

47
EFFICACY AND SAFETY OF MK-5172 AND
MK-8742 ± RIBAVIRIN IN HCV GT1
INFECTED PATIENTS WITH CIRRHOSIS OR
PREVIOUS NULL RESPONSE:
FINAL RESULTS OF THE
C-WORTHY STUDY (PARTS A AND B)
Eric Lawitz, Edward J. Gane, Brian Pearlman, Edward Tam, Wayne
Ghesquiere, Dominique Guyader, Laurent Alric, Jean-Pierre
Bronowicki, Laura Lester, William Sievert, Reem H. Ghalib, Luis A.
Balart, Fredrik Sund,
Martin Lagging, Frank Dutko, Anita Y. M. Howe,
Melissa Shaughnessy, Peggy Hwang, Janice Wahl,
Michael Robertson, Eliav Barr, Barbara Haber

48
BACKGROUND
C-WORTHy: Grazoprevir + Elbasvir ± RBV in 471 HCV GT1-infected
patients Treatment-naive, non-
cirrhotic 12 weeks ± RBV
(n = 65) Pt. A
Treatment-naive Non-cirrhotic
8-12 weeks ± RBV (n = 94) Pt.B
Treatment-naive Cirrhotic
12-18 weeks ± RBV (n = 123) Pt. B
HIV/HCV Co-infected Non-cirrhotic
12 weeks ± RBV (n = 59) Pt.B
Null Responders Cirrhotic / Non-cirrhotic
12-18 weeks ± RBV (n = 130) Pt. B

49
C-WORTHY
TREATMENT-NAÏVE CIRRHOTICS AND NULLS
Key eligibility criteria:
≥18 years old with chronic HCV GT1a or GT1b infection
Treatment-naïve to prior HCV therapy or,
Null response to prior PR (<2 log10 decline from baseline in HCV
RNA after 12 weeks)
Cirrhosis based on either liver biopsy or noninvasive test
HIV and HBV negative
ALT and AST <350 IU/L
Albumin ≥3.0 g/dL; platelets ≥70,000/mm3
49

50
SVR12 RATES IN SUBGROUP
ANALYSIS
Subgroup
No Cirrhosis
Cirrhosis
Tx-naïve
Null Responders
HCV RNA >2 million
HCV RNA ≤2 million
GT1b
GT1a
> 50 years
≤ 50 years
18 weeks
12 weeks
Overall SVR12=93% No RBV
+ RBV
0
N
41
42
84
86
60
63
65
65
100
92
25
36
41
46
82
81
102
99
23
29
63
65
62
63
70 80 90 100 % SVR12 (Mean; 95% CI)

51
EFFICACY WITH 12 OR 18 WEEK REGIMENS
GRAZOPREVIR AND ELBASVIR ± RBV*
* Includes all patients treated with 12 or 18 weeks of grazoprevir + elbasvir ± RBV
95 94 93 99
94 95 95 95
0 10 20 30 40 50 60 70 80 90
100
SVR
12
(%
)
122
128
116
123
86
87
152
163
118
125
79
83
161
170
124
130
SVR12 was 92% (23/25) in null
responders with cirrhosis
treated
for 12 weeks with grazoprevir +
elbasvir ± RBV

52
COMMON ADVERSE EVENTS
DURING TREATMENT
* incidence ≥10% in All Patients;
order in decreasing frequency based on All Patients
Common Adverse Event*
All Patients n = 253
Treatment-naïve + Cirrhosis
PR-Null ± Cirrhosis
+ RBV n =63
No RBV n = 60
+ RBV n=65
No RBV n=65
Fatigue 66 (26%) 14 (22%) 14 (23%) 15 (23%) 23 (35%)
Headache 58 (23%) 7 (11%) 21 (35%) 15 (23%) 15 (23%)
Asthenia 35 (14%) 3 (5%) 7 (12%) 12 (18%) 13 (20%)

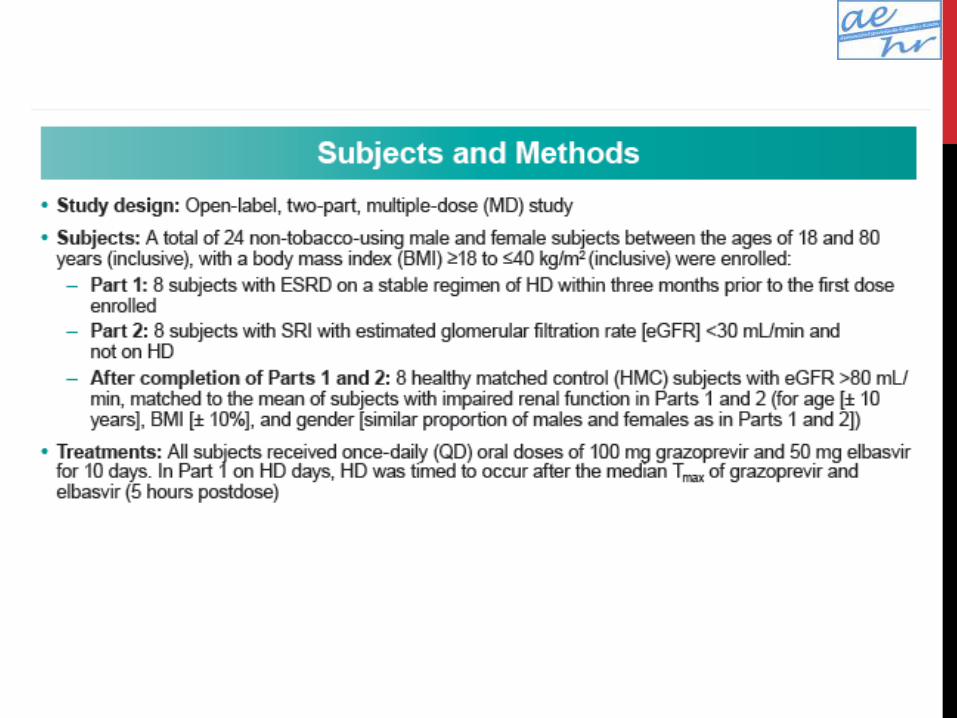
PHARMACOKINETICS OF CO-ADMINISTERED
GRAZOPREVIR AND ELBASVIR IN VOLUNTEERS
WITH ESRD ON HEMODIALYSIS OR PREDIALYSIS

FARMACOCINÉTICA:
CONCLUSIONES
• La coadministración de grazoprevir y elbasvir fue en
general bien tolerada en los sujetos en HD y con ERCA
• La HD no afecta a la farmacocinética de manera
significativa
• Muy alta unión a proteínas (sobre todo elbasvir)
• Las concentraciones de grazoprevir y elbasvir fueron
mayores en los sujetos con ERCA sin HD vs sanos
• La disfunción renal influye en la eliminación hepática por
los altos niveles de toxinas urémicas, PTH y citoquinas
que pueden inhibir los citocromos y transportadores
hepáticos

ENSAYO CLÍNICO MK-
5172 + MK-8142
• C-WORTHY part B
• Genotipo 1 ± cirrosis
• Genotipo 1, VIH+, no cirrosis
• C-SCAPE
• Genotipos 2, 4-6
• C-SALVAGE
• No respuesta previa a otros IPs (boce/tela, sime/sofos)
• Fase II/III en poblaciones especiales
• ERC 4-5D
• Child-Pugh B con cirrosis
• C-EDGE
• Fase III en genotipos 1, 4-6: naïve/no respondedor, cirrosis/no cirrosis, VIH+/-

C-SURFER:
CRITERIOS DE INCLUSIÓN
• 210 pacientes naïve y recaedores +/- cirrosis (no cirróticos en
Europa)
• ERC 4-5 y en hemodiálisis (incluidos trasplantados previos)
• Ensayo clínico controlado, randomizado, en paralelo,
multicéntrico, con placebo
• Objetivos:
• Evaluar la eficacia en sujetos VHC+ genotipo 1 con ERC
• Evaluar la seguridad y tolerancia

C-SURFER:
CRITERIOS DE EXCLUSIÓN
• Diálisis peritoneal
• Hepatopatía descompensada
• Coinfección VHB/VIH
• Neoplasias < 5 años
• Abuso de tóxicos
• Gestantes o en lactancia
• Antecedentes cirugía gástrica o enfermedades malabsortivas
• Corticoterapia (prednisona ≥ 10 mg/24 h)
• Evento cardiovascular < 3 meses
• Analíticos
C-SURFER:
MEDICACIÓN
Posología
• MK-5172, 100 mg al día (grazoprevir)
• MK-8142, 50 mg al día (elbasvir)
Duración
• 12 semanas
• 24 semanas si grupo placebo previo
Efectos secundarios: anodinos
Eficacia estimada: (basada en ensayos de no renales)

MK-5172 100 mg
+
MK-8742 50 mg
FU Follow-up
MK-5172 placebo
+
MK-8742 placebo
FU
MK-5172 100 mg
+
MK-8742 50 mg
Follow-up
D1 W12 W16 W28 W36 W52
Immediate tr. arm
n=105
Deferred tr. arm
n=105
Blinded period Open label period
C-SURFER (N=210)
PARTICIPANTES C-SURFER
• España
• Hospital La Mancha-Centro
(coordinador europeo)
• Hospital 12 de Octubre
• Hospital Clìnic
• Suecia
• Francia
• Países Bajos
• Reino Unido
• Estados Unidos
• Estonia
• Lituania
• Israel
• Australia
• Argentina
• Corea
• Canadá

NUESTRA EXPERIENCIA
PACIENTE TTO PREVIO ENSAYO RV8 RVS
Paciente 1 Relapser MK sí sí
Paciente 2 Relapser Placebo
Paciente 3 Relapser MK sí sí
Paciente 4 Naïve Placebo
PACIENTE CRITERIO DE EXCLUSIÓN
Paciente 5 Hemodiálisis < 3 meses
Paciente 6 Pie diabético
Paciente 7 No genotipo 1
Paciente 8 Renuncia tras cribado
Paciente 9 Cirrosis
Paciente 10 Hb < 9 g/dl

EVENTOS ADVERSOS
MK
Astenia
Celulitis
Náuseas
Eritema no pruriginoso
Dolor articular en muñecas
Inflamación tarsos
Neutropenia afebril
Vómitos
Alopecia
Mareo
PLACEBO
Febrícula
Anorexia
Vómitos
Dolor articular generalizado
Insomnio
Ansiedad

QUALITY OF LIFE
• When compared to IFN and RBV-containing regimens, HRQOL
was not negatively impacted during treatment with grazoprevir
+ elbasvir
• In contrast, HRQOL was greatly reduced during treatment with
the IFN/RBV-containing regimen; this was most likely
associated with the adverse event profile of IFN/RBV

• ¿TRATAMIENTO DE VHC
CRÓNICA ANTES DEL
TRASPLANTE RENAL?
CONCLUSIONES

Unidad Hepatorrenal
