microbiological diagnosis of tb josé domínguez 1 and sabine rüsch-gerdes 2 1 servei de...
TRANSCRIPT

Microbiological diagnosis of TB
José Domínguez1 and Sabine Rüsch-Gerdes2
1Servei de Microbiologia. Fundació Institut en Ciències de la Salut Germans Trias i Pujol. Badalona. Spain
2 Forschungszentrum Borstel, National Referencelaboratory for Mycobacteria. Borstel.
Germany

Microbiological diagnosis of TB:Detection, identification and
molecular epidemiology
José DomínguezServei de Microbiologia.
Fundació Institut en Ciències de la Salut Germans Trias i Pujol
One of the main objectives for TB control
“Diagnosis, diagnosis & diagnosis”William Osler
HistologyClinical suspicion Microbiology
Objectives for TB control
•To rapidly diagnose patients with active TB and treat them correctly.
•To have rapid diagnostic methods, with high sensitivity and specificity to diagnose diseased patients at the beginning of the symptoms for an adequate treatment prescription
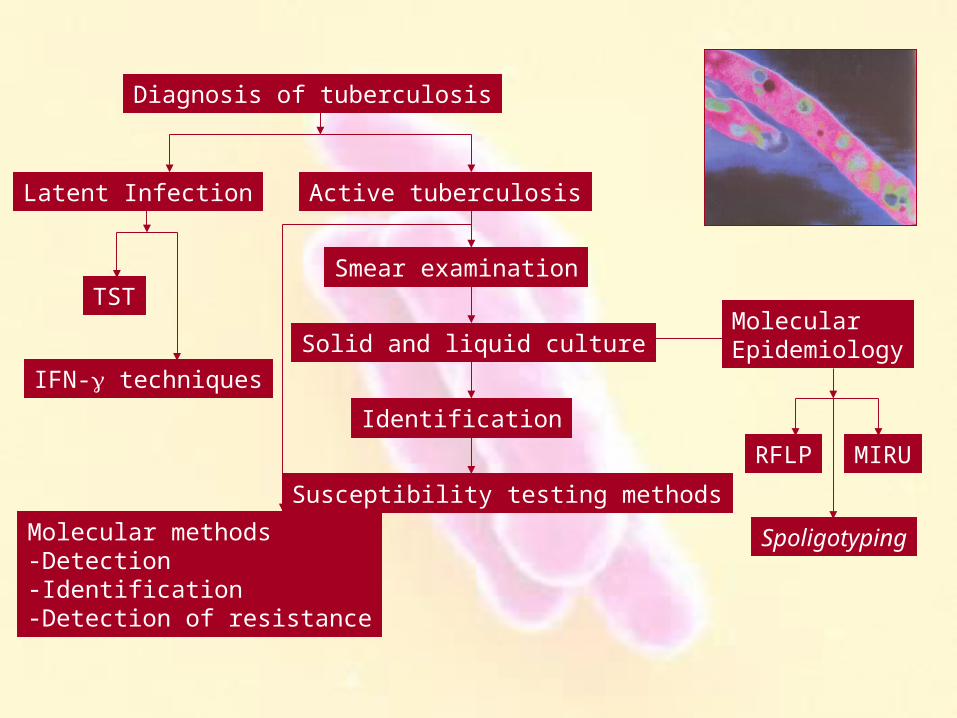
Diagnosis of tuberculosis
Latent Infection Active tuberculosis
Smear examination
Solid and liquid culture
Identification
Susceptibility testing methods
TST
IFN- techniques
MolecularEpidemiology
RFLP
Spoligotyping
MIRU
Molecular methods-Detection-Identification-Detection of resistance

Clinical samples
Samples!! Respiratory and extra-respiratory
Quantity: high inoculums means fast growthQuality, including sputum, high yieldLocalization, biopsies when possible
Rapid shipmentPrevious to starting treatment
Think of histology
The most important:Clinical-Microbiologist-Pathologist Communication

Decontamination
• Eliminate normal flora from the non-sterile samples (micobacteria is acid and alkaline resistant)• Homogenization to release the bacteria from the sample and allow access to the nutrient present in the media
i.e. KubicaN-acetyl-cysteine: homogenizationNaOH: decontaminantNeutralization by phosphate buffer
Homogenization
Sample mixing
Phosphate buffer
Centrifugation
Pellet

Smear microscopy
Ziehl-Neelsen stain Auramina O stain
Fast; Cheap; Monitorization of treatment; Low sensitivity
Hospital Univ. Germans Trias i Pujol 2004 -2007 Pulmonary Disseminated Extrapulmonary*
TOTAL 125 18 60
Positive smear 83 (66.4%) 11 (61.1%) 11 (18.3%)
Negative smear 42 (33.6%) 7 (38.9%) 49 (81.7%)
*Adenopathy, 4/28 (14.2%); Pleural, 1/17 (5.9%)
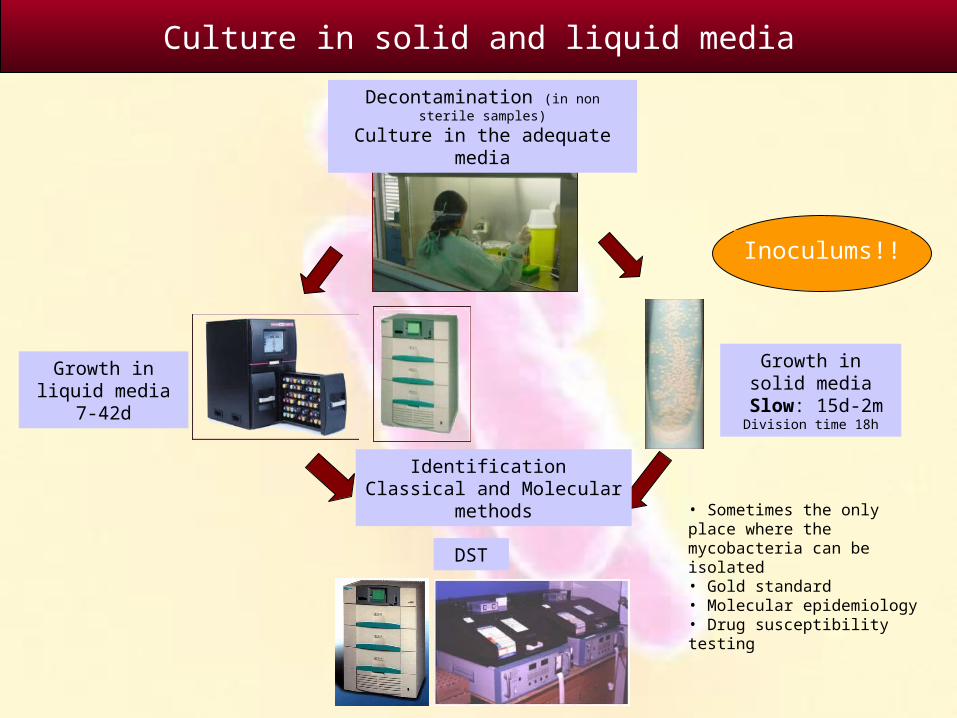
Decontamination (in non sterile samples)
Culture in the adequate media
Culture in solid and liquid media
• Sometimes the only place where the mycobacteria can be isolated• Gold standard• Molecular epidemiology• Drug susceptibility testing
DST
Growth in solid media
Slow: 15d-2mDivision time 18h
Growth in liquid media7-42d
Inoculums!!
Identification Classical and Molecular
methods
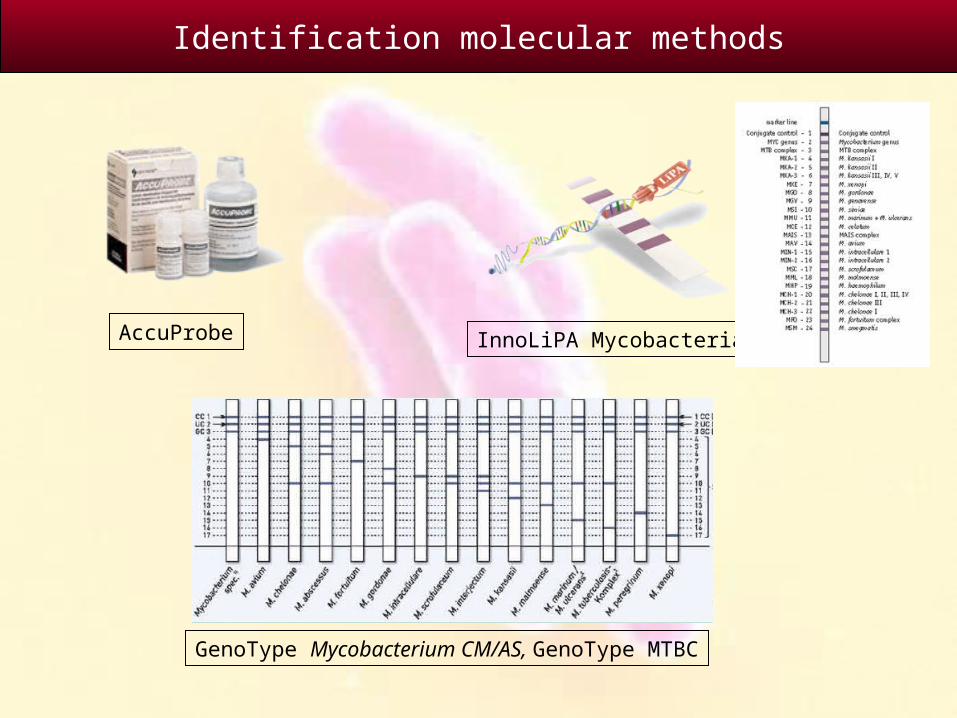
Identification molecular methods
InnoLiPA MycobacteriaAccuProbe
GenoType Mycobacterium CM/AS, GenoType MTBC
Identification molecular methods
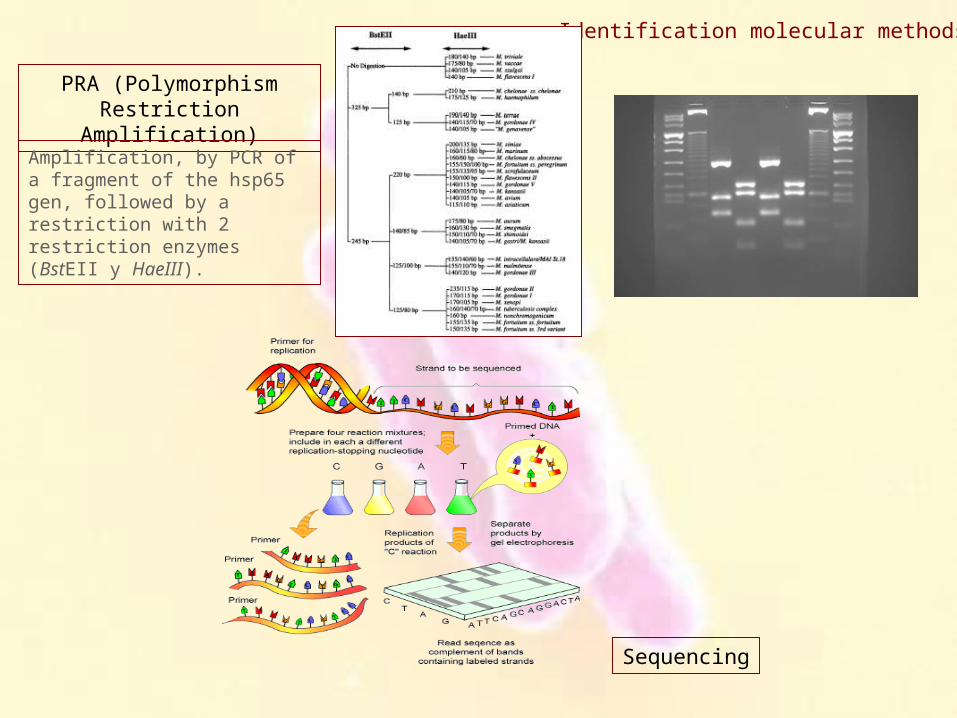
Sequencing
PRA (Polymorphism Restriction Amplification)
Amplification, by PCR of a fragment of the hsp65 gen, followed by a restriction with 2 restriction enzymes (BstEII y HaeIII).
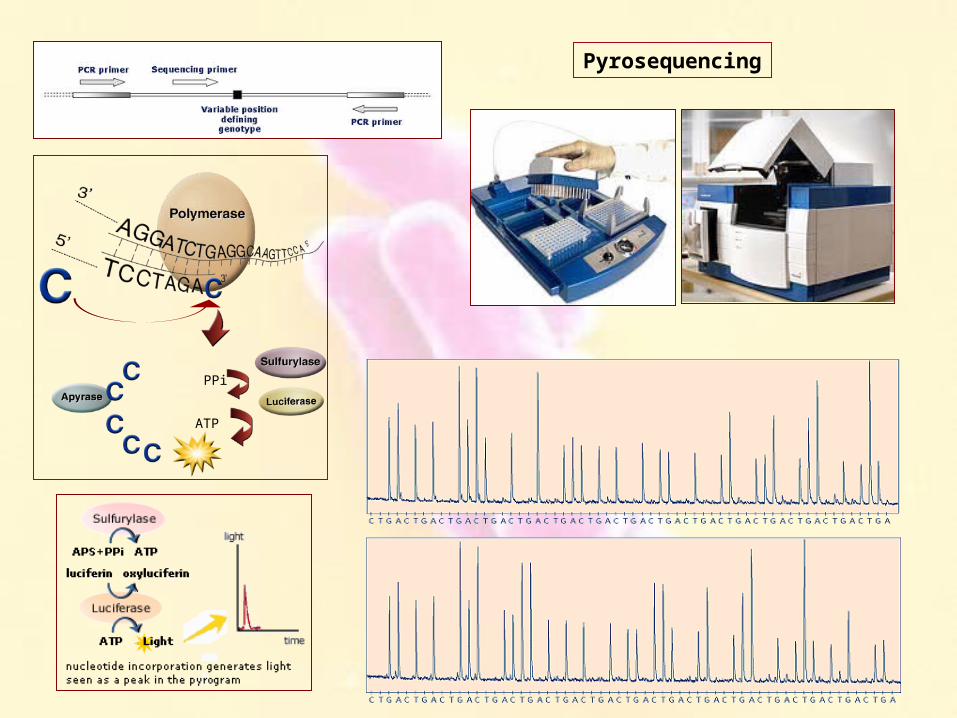
Pyrosequencing
PPi
ATP


M.tuberculosis detection in clinical samples by molecular methods
Method Target Detection methodSensitivity in respiratory samples (%)
Sensitivity inextra respiratory
samples (%)
Overall specificity
(%)
AMTD2 16S rRNA Chemiluminometric 80-100 60-90 95-100
LCx b antigenic protein Fluorimetric 80-90 65-80 90-100
AMPLICOR 16S rRNA Colorimetric 75-100 45-60 90-100
BD ProbeTecIS6110 and16S rRNA
Fluorimetric 55-100 30-80 45-100
INNO-LIPA v2 IR16S-23S Colorimetric 50-95 60-80 90-100
GenoType Direct
23S rRNA Colorimetric 60-95 60-80 95-100
PCR real time 16S rRNA Fluorimetric 70-90 65-85 85
* In smear negative samples the sensitivity is reduced in a 50%
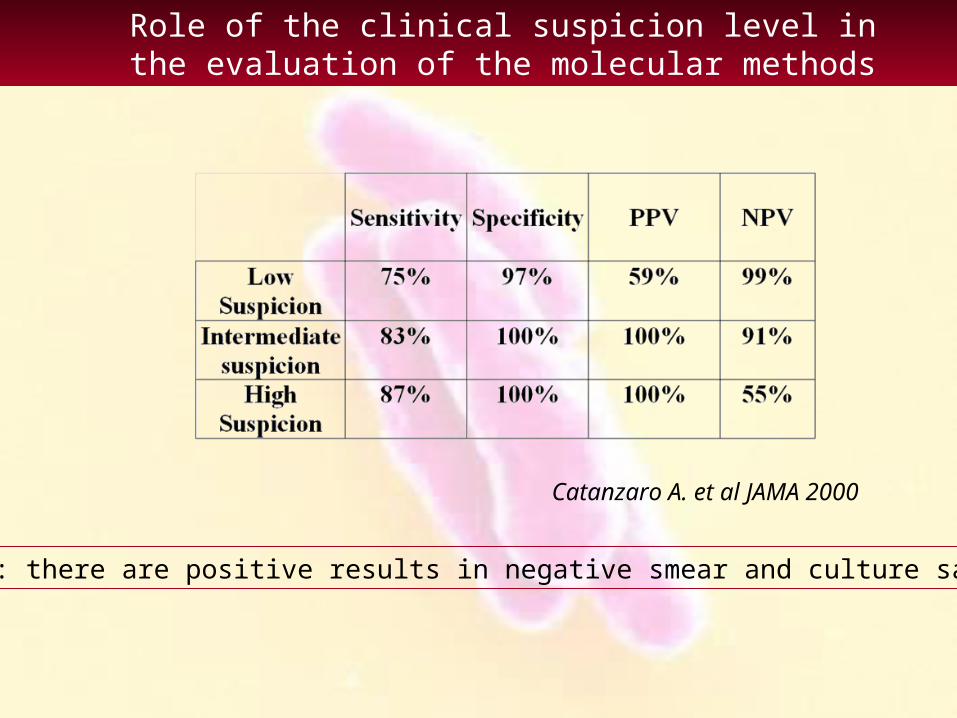
Role of the clinical suspicion level inthe evaluation of the molecular methods
Catanzaro A. et al JAMA 2000
Problem: there are positive results in negative smear and culture samples.
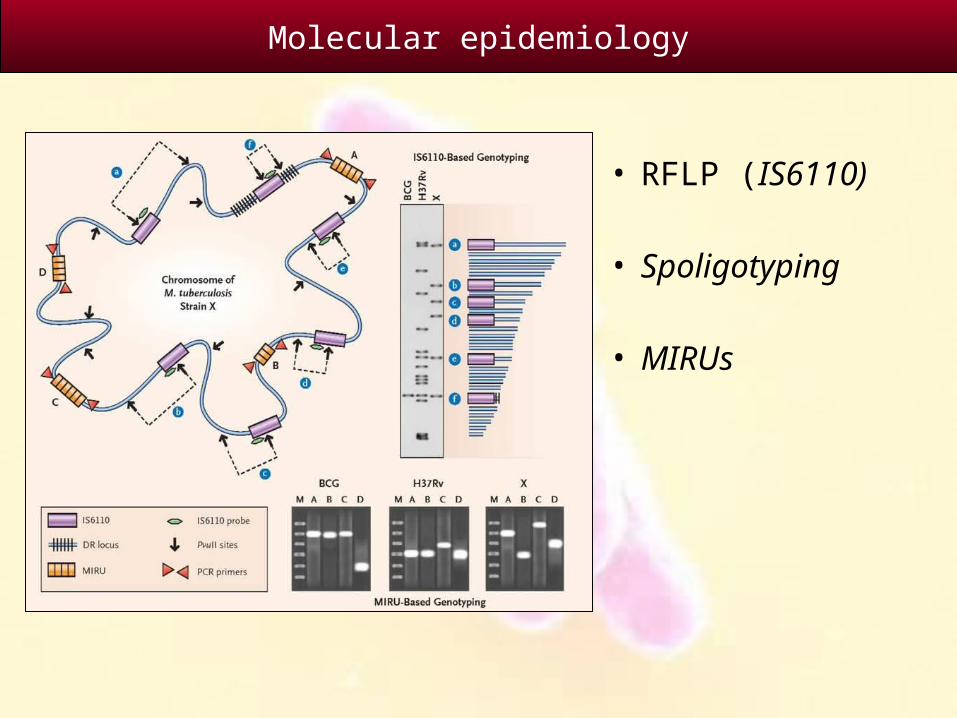
• RFLP (IS6110)
• Spoligotyping
• MIRUs
Molecular epidemiology
• Insertion sequence present exclusively in the M.tuberculosis complex: IS6110
• High polymorphism between no related strains regarding the number of copies and their localization in the chromosome.
• Advantages: High discriminative power.• Disadvantages: Slow, laborious and with
certain complexity.
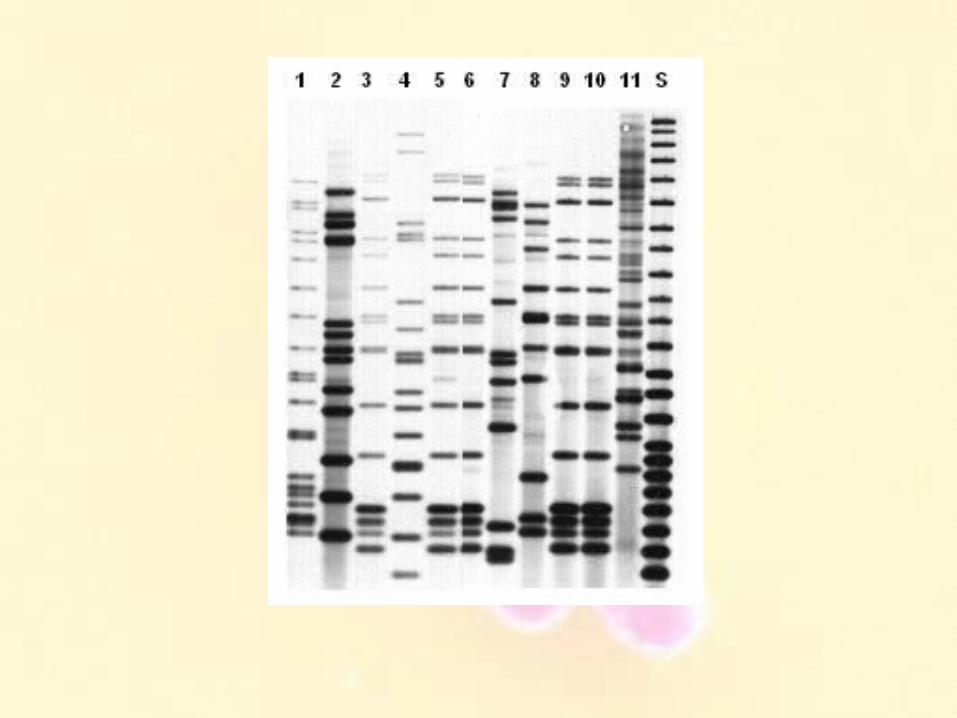
Restriction Fragment Length Polymorphism (RFLP)

Electrophoresis
Pvu II
Extraction and restriction
Hybridization
Transference
Radiographic develop

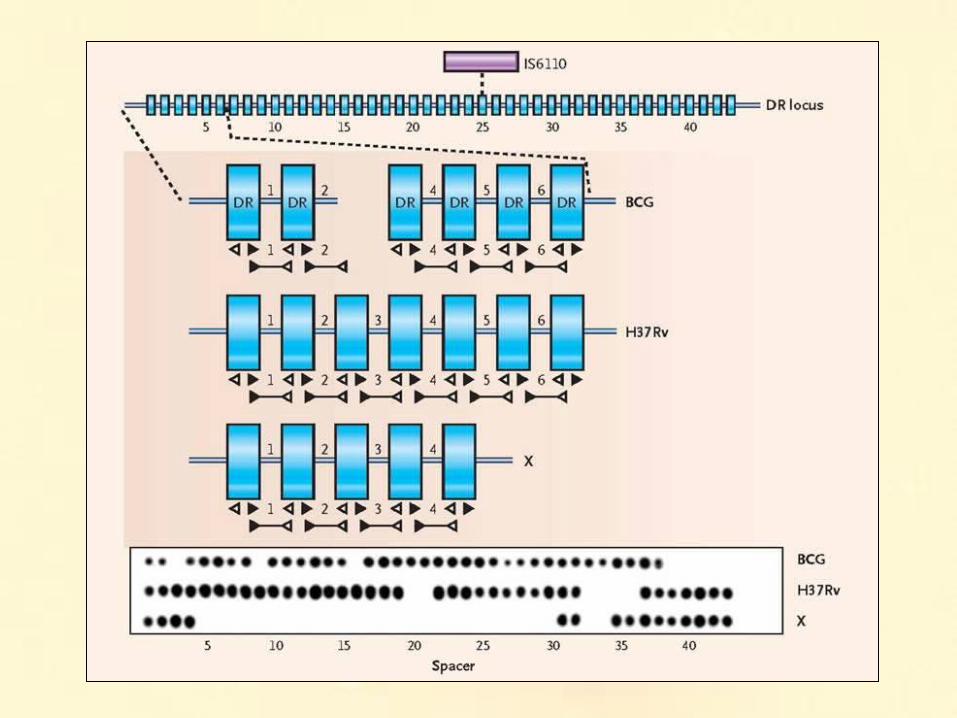
• The DR sequences (direct repeat) are repeated sequences of 36 bp in only one locus of the M.tuberculosis chromosome, separated by sequences of 34 to 41 bp.
• The technique is based on a PCR of the locus where the DR sequences are located. The amplification product is hybridized with oligos synthesized from the inter-DR spaces.
• The presence or absence of different DR allows a specific pattern for each strain.
• Advantages: Few DNA is required, easy interpretation• Disadvantages: Lesser discriminative power than the
RFLP.
Spacer oligonucleotype typing (Spoligotyping)

• Determine the number of repetitive units in 12 (15 or 20) different locus of one genetic sequence called “mycobacterial interspersed repetitive units (MIRUs)”. The number of repetitions is detected by PCR.
• The number of repetitive units in each locus is calculated by the size of the fragment amplified with the specifics primers.
• MIRU-VNTR is more discriminative than the spoligotyping and similar to the RFLP-IS6110.
• Advantages: rapid, simple and automatic.• Disadvantages: In study
Micobacterial Interspersed Repetitive Units (MIRU)

Micobacterial Interspersed Repetitive Units (MIRU)
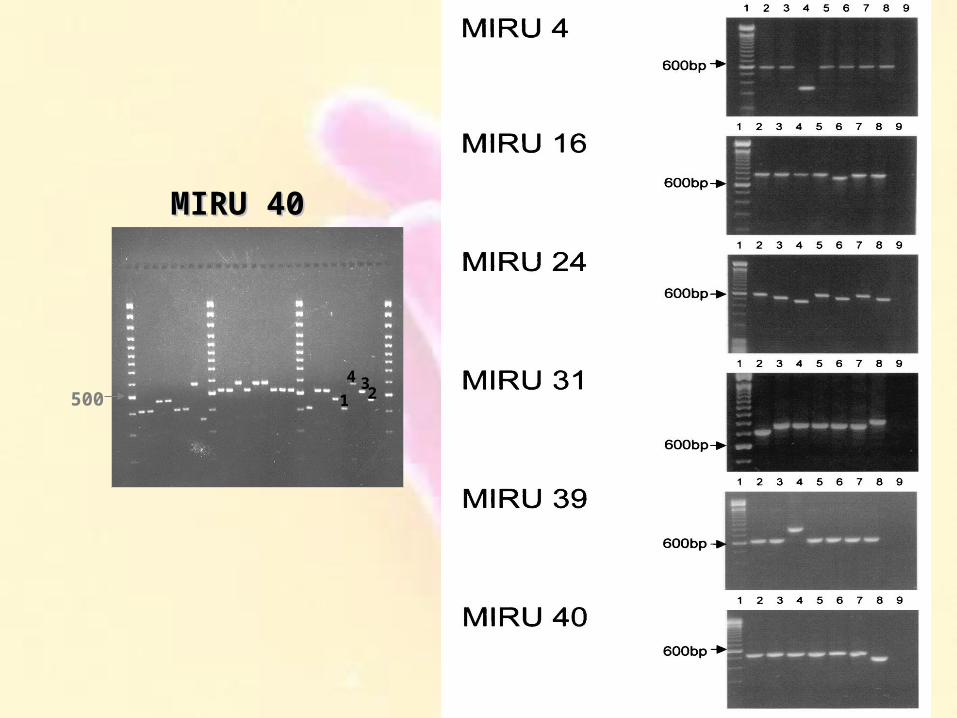
MIRU 40 MIRU 40
500
pb
1
4 32
• The microbiological diagnosis of TB will be rapid and accurate if adequate samples are collected and adequate inoculums are used. Don’t forget histology.
• The future of TB diagnosis remains in the application of new molecular techniques but, at the moment a cautious interpretation of the results is required.
• The sensitivity of the molecular tests vary, and is affected by the amount of bacteria present in the samples, and also by the clinical suspicion level. Low sensitivity is present in samples with low bacterial load, especially in extra respiratory samples.
• At the moment, new molecular methods can not substitute the conventional ones. The gold-standard is the culture, and the other methods have to be considered and interpreted as complementary diagnostic methods.
• Communication between clinicians and microbiologists is imperative.
Conclusions
National Reference Laboratory for Mycobacteria
Forschungszentrum Borstel
Sabine Rüsch-Gerdes
Microbiological Diagnosis of TBDrug Susceptibility Testing
Borstel 2010

Drug Susceptibility Testing

MDR TB – New Infection
WHO: MDR-TB & XDR-TB, The 2008 Report; February 2008
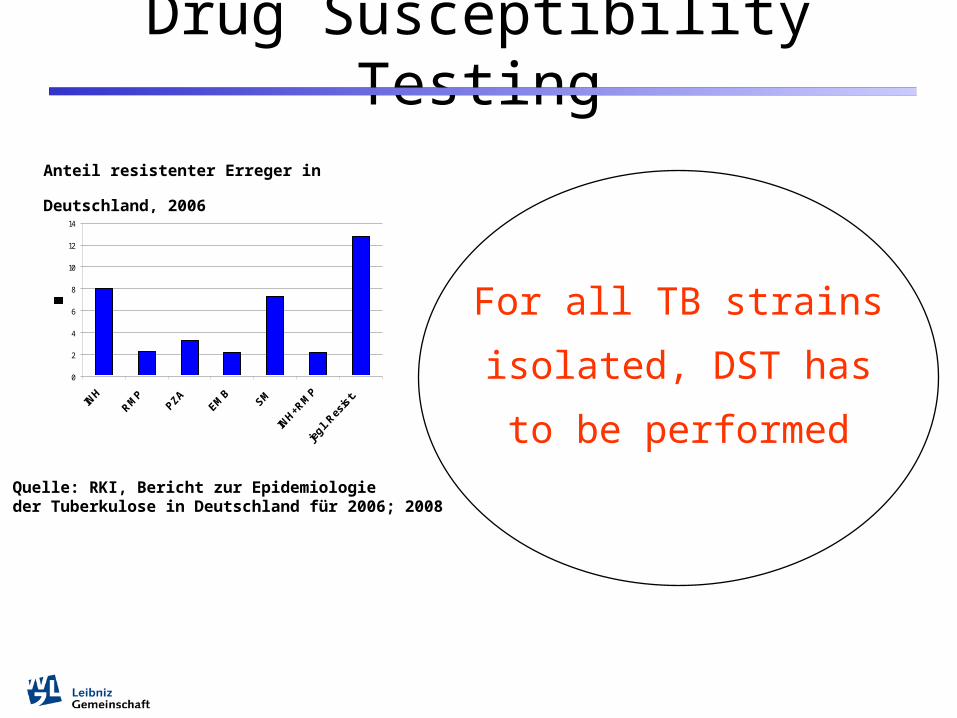
Drug Susceptibility Testing
For all TB strains
isolated, DST has to be
performed
Anteil resistenter Erreger in Deutschland,
2006
0
2
4
6
8
10
12
14
Quelle: RKI, Bericht zur Epidemiologie der Tuberkulose in Deutschland für 2006; 2008
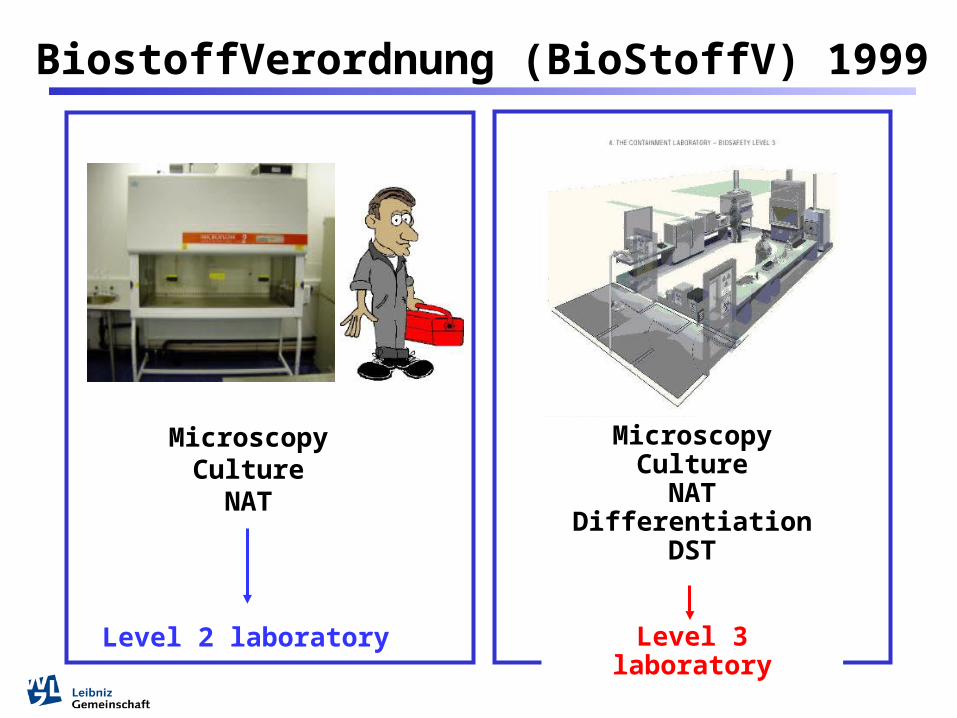
MicroscopyCulture
NATDifferentiation
DST
Level 3 laboratory
MicroscopyCulture
NAT
BiostoffVerordnung (BioStoffV) 1999
Level 2 laboratory
Proportion method on Löwenstein-Jensen medium
H, R, E, S, PTH, CM, OFL, CS, NSA (instead of P)
Results available:4-6 weeks
No critical concentrations for new substances
Methods for Drug Susceptibility Testing

BACTEC 460TB All drugs except cycloserine
Methods for Drug Susceptibility Testing
Results available:1-2 weeks
Radioactive materials, waste

Results available:
1-2 weeks
Methods for Drug Susceptibility Testing
MGIT 960 For all drugs, except CS
Advantages compared to solid media:• more rapid• high quality of media• fully automated system• testing of 1st, 2nd, and new drugs• safety: plastic tubes
Disadvantages:• expensive• higher contamination rate• dependency on a company• no DST for Cycloserine
Liquid media compared to solid media
Infection control strategies
Proposed measures:
• Improved ventilation system• Reduced hospitalsation• Mask use• Isolation of patients• HIV-testing and therapy• Rapid drug-susceptibility testing
Time for the detection has a potential to reduce the extend of spread of resistant strains
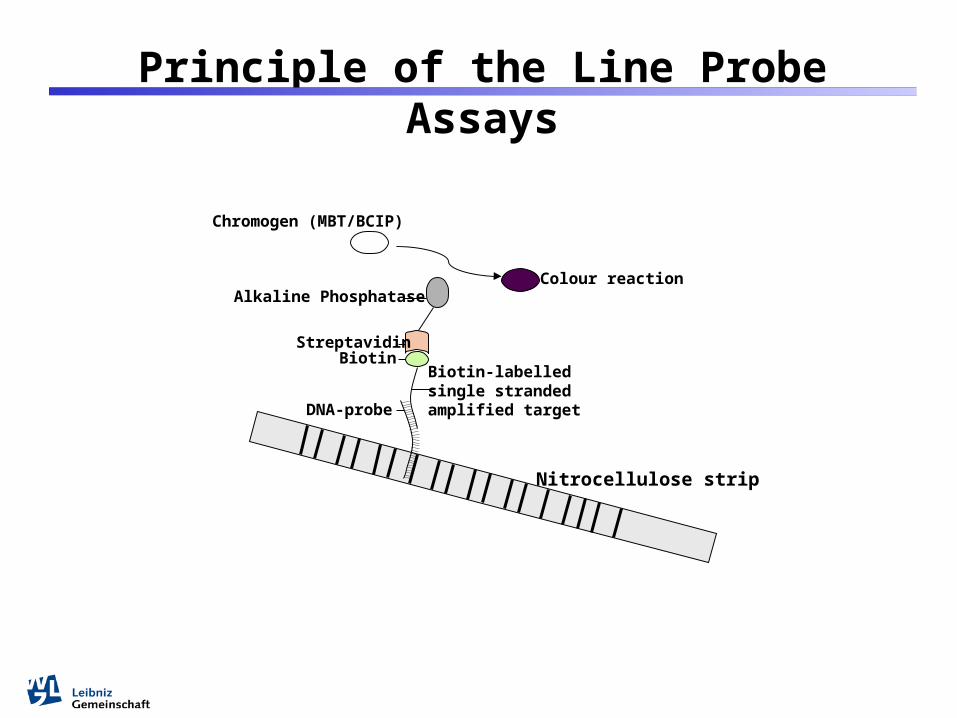
Principle of the Line Probe Assays
Chromogen (MBT/BCIP)
Alkaline Phosphatase
StreptavidinBiotin
Nitrocellulose strip
DNA-probe
Biotin-labelled single stranded amplified target
Colour reaction

Control of the conjugate -
Amplification control - Amplification control
MTBC - Control rpoB -
rpoB Wild type 1 - rpoB Wild type 2 - rpoB Wild type 3 -rpoB Wild type 4 -rpoB Wild type 5 -rpoB Mut D516V -rpoB Mut H526Y -rpoB Mut H526D -rpoB Mut S531L -
Control katG -katG wild type -
katG S315T1 (ACC) -katG S315T2 (ACA) -
1 2 3 4 5 6 7 8
MTBDR – DNA Hybridisation Strip

1 2
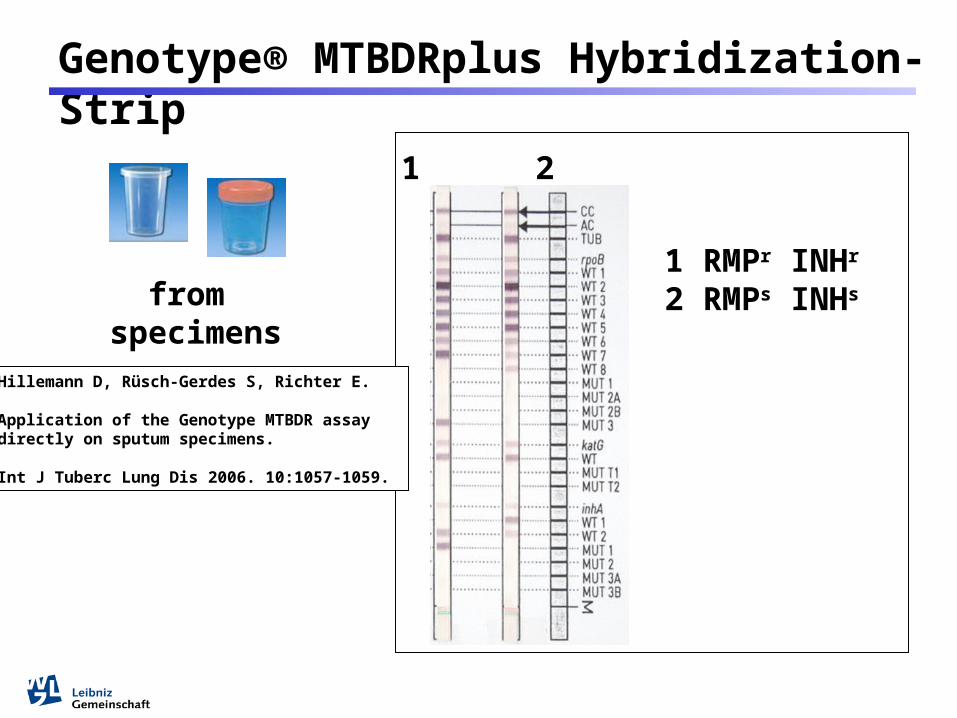
Genotype® MTBDRplus Hybridization-Strip
1 RMPr INHr
2 RMPs INHs
fromCulture media

Results RMP+INH Resistance
100 % concordance between sequencing and MTBDR data
103 MDR strains
91 strains (88.4) with mutations in codon 315 of
katG
102 strains (99%) mutations in rpoB cluster
I
1 strain (1%) a mutation outside rpoB
cluster I
3 strains (2,9 %) with a mutation in inhA
+2 strains (1,9 %)
with a mutation in ahpC+
7 strains (6,8 %) with no mutation in katG, inhA and
ahpC
1 strain (1%) not detected as MDR (rpoB outside cluster I, ahpC)
+
+
+
1 2
Genotype® MTBDRplus Hybridization-Strip
1 RMPr INHr
2 RMPs INHsfrom specimens
Hillemann D, Rüsch-Gerdes S, Richter E.
Application of the Genotype MTBDR assaydirectly on sputum specimens.
Int J Tuberc Lung Dis 2006. 10:1057-1059.
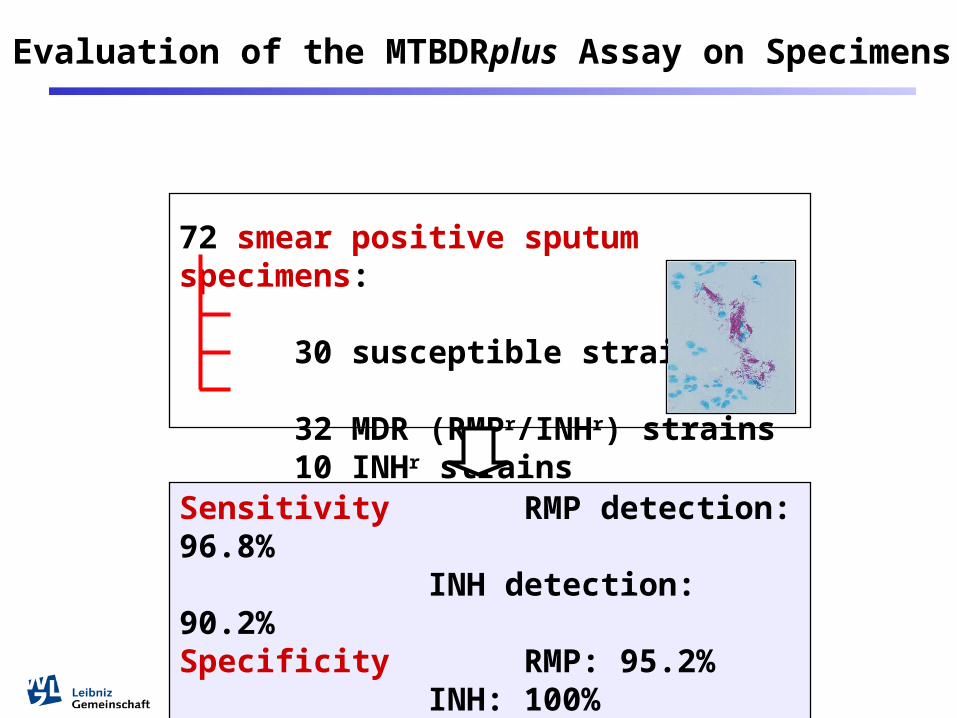
Evaluation of the MTBDRplus Assay on Specimens
72 smear positive sputum specimens:
30 susceptible strains 32 MDR (RMPr/INHr) strains 10 INHr strains
Sensitivity RMP detection: 96.8%
INH detection: 90.2%Specificity RMP: 95.2%
INH: 100%

Line Probe Assays for DST
INNO-LiPA Rif TB
GenoType MTBDRplus
GenoType MTBDRsl
Resistance Sensitivity Specificity
RMP 98.1% 98.7%
INH 84.3% 99.5%
Ling et al., Eur Respir J 2008
Evaluated line probe assays
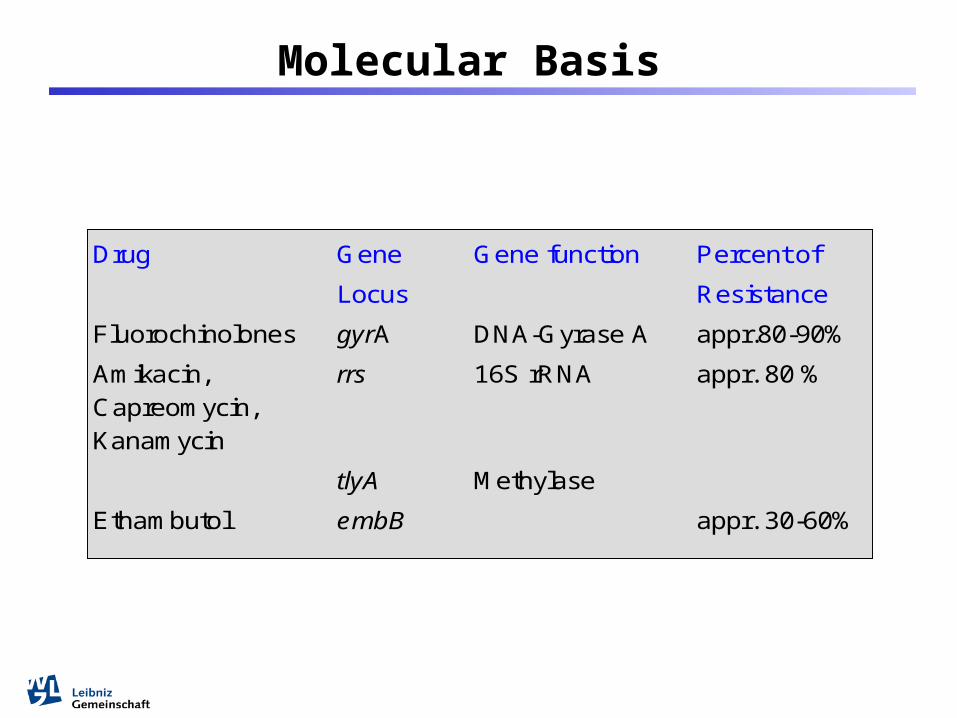
Molecular Basis
Drug Gene
Locus
Gene function Percent of
Resistance
Fluorochinolones gyrA DNA-Gyrase A appr.80-90%
Amikacin, Capreomycin, Kanamycin
rrs 16S rRNA appr. 80 %
tlyA Methylase
Ethambutol embB appr. 30-60%
• Overall sensitivity for OFL, AM, CM and EMB was 90.2 %, 83.3 %, 86.8 % and 59.0 %, respectively.
• Specificity was 100 % for FLQ, AM, and EMB, and 99.1 % for CM.
• Most prevalent mutations were:gyrA D94G in Oflr strainsrrs A1401G AMr/CMr strains embB M306V in EMBr strains
• The rapid detection of XDR strains is possible with the combined application of Lipas from DNA isolates and directly from sputum specimens.
Summary
Time-to-result: 1 h 45 min
GeneXpert
FIND 2009
Xpert MTB
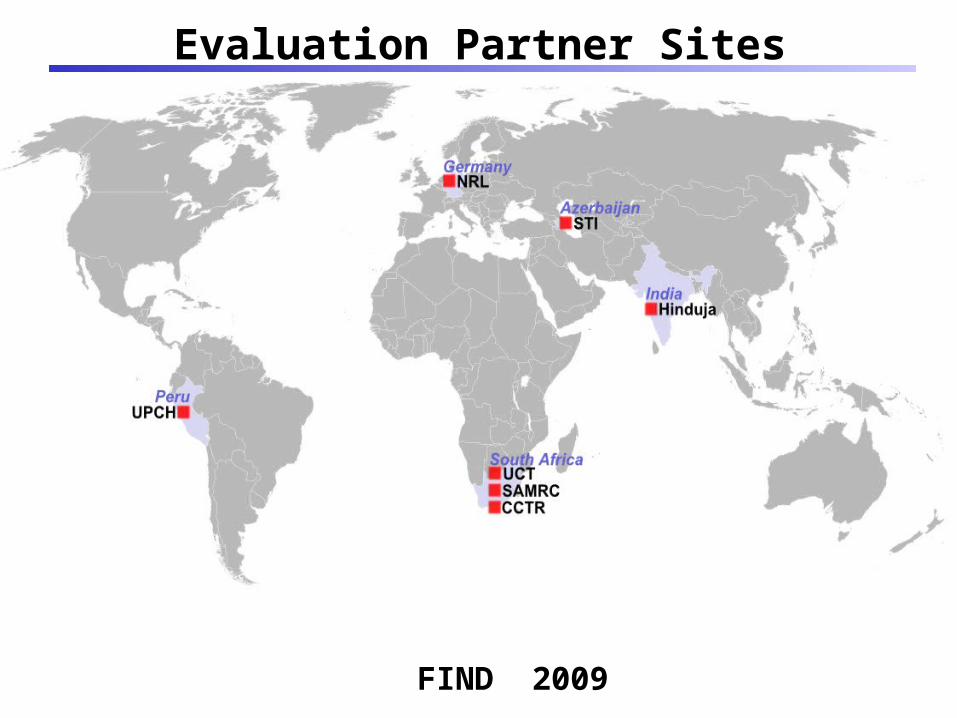
Evaluation Partner Sites
FIND 2009

High tech for low tech settings:
Sensitivity and Specificity seems to be very good for the detection of TB and Rifampicin resistance.
Xpert MTB

Drug Susceptibility Testing
7 - 10 days
3 - 4 weeksSolid MediaLöwenstein-Jensen(Middlebrook)
Liquid MediaBACTEC 460 TBMGIT
Molecular based MethodsInnoLipaGenoTypeMTBDRXpert MTB‚home made‘- methods
Hours – 1day
Quality Control
internal external
Internal Quality Control
all reagents
all techniques
all staffs

All QC results have to be documented
Internal Quality Control
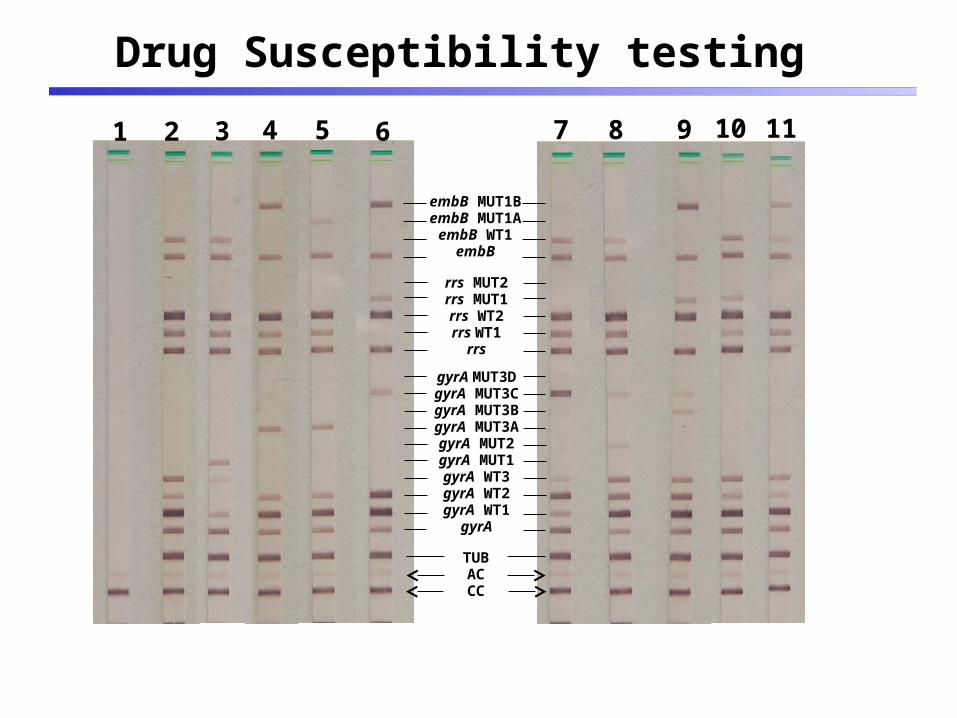
1 2 3 4 5 6 7 8 9 10 11
embB MUT1BembB MUT1A
embB WT1embB
rrs MUT2rrs MUT1rrs WT2rrs WT1
rrs
gyrA MUT3DgyrA MUT3CgyrA MUT3BgyrA MUT3AgyrA MUT2gyrA MUT1gyrA WT3gyrA WT2gyrA WT1
gyrA
TUBACCC
Drug Susceptibility testing

External Quality Control
Participation in international QA programs

Reliable results
To detect and treat patients properly