enfermedades autoinmunes sistémicas martes, 13 de ... fileser 7,5 mg/d) bajar las dosis muy ......
TRANSCRIPT
Enfermedades autoinmunes sistémicas martes, 13 de noviembre de 2012
Patricia E Carreira Médico adjunto de reumatología Hospital Universitario 12 de Octubre, Madrid

Polimialgia reumática y arteritis de células gigantes M Cinta Cid
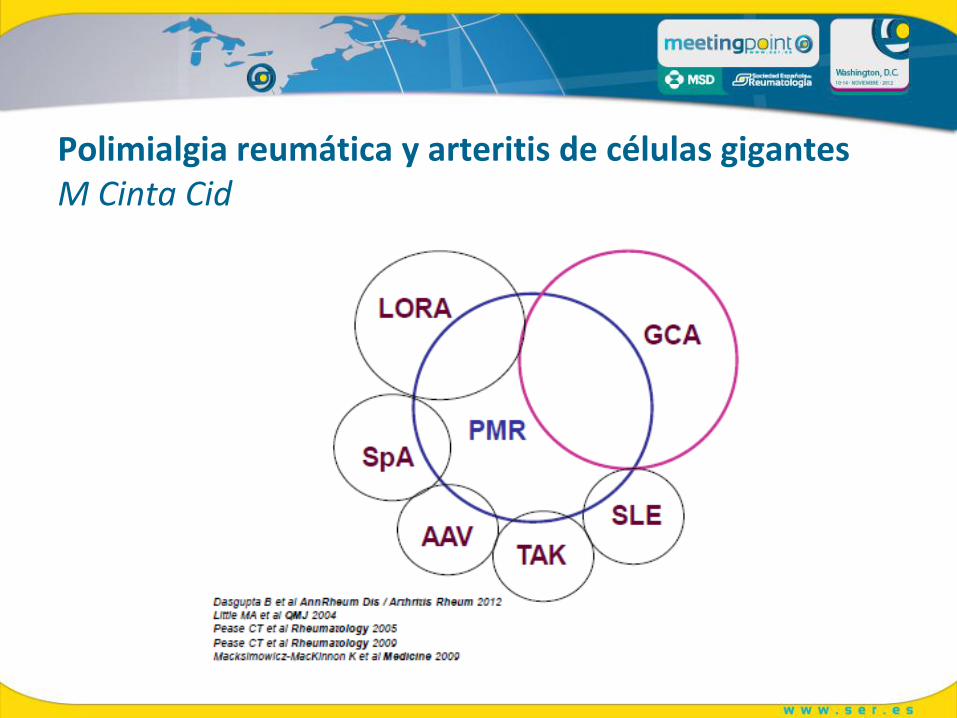
Polimialgia reumática y arteritis de células gigantes M Cinta Cid
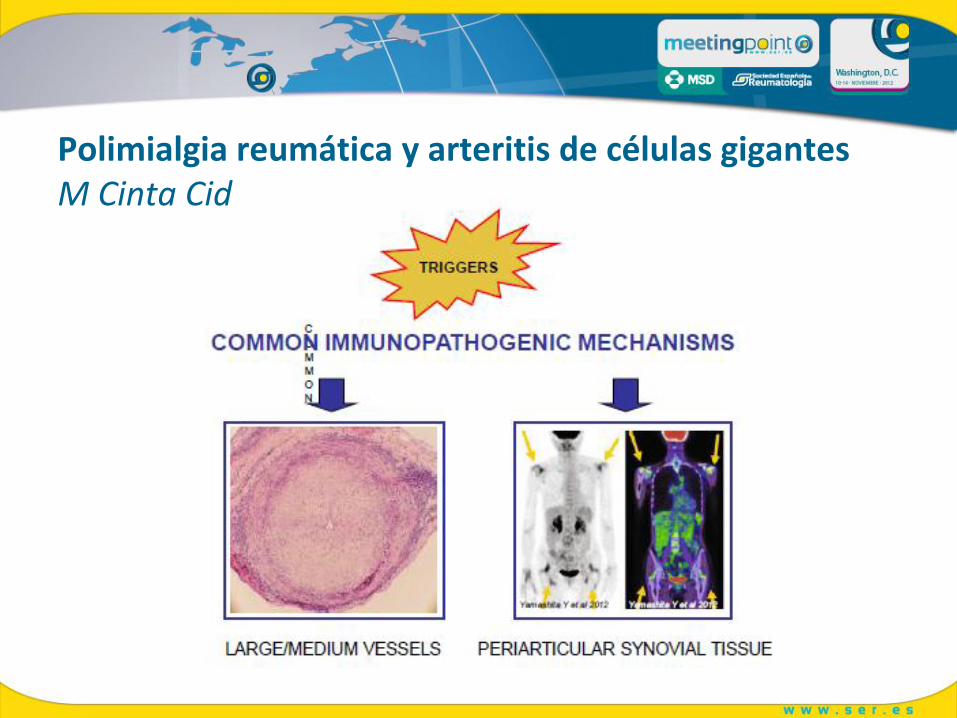
Polimialgia reumática y arteritis de células gigantes M Cinta Cid
Polimialgia reumática, tratamiento Carlo Salvarani
Glucocorticoides: ”KEY POINTS” Iniciar la dosis más pequeña posible (15 mg/d es habitualmente suficiente, en casos más leves pueden ser 7,5 mg/d) Bajar las dosis MUY LENTAMENTE: a partir de 7,5 mg, disminuir 1 mg/d al mes No siempre que aumenta la VSG o la PCR significa actividad El tratamiento debe adaptarse al paciente

Polimialgia reumática, tratamiento Carlo Salvarani
Ahorradores de glucocorticoides Metotrexate: no eficaz (al menos a 15 mg/sem) Infliximab, Etanercept: no eficaces
Polimialgia reumática, tratamiento Carlo Salvarani
Terapias futuras: Anti-IL6 (Tocilizumab) MTX a dosis más altas? Leflunomida Anti-CD20?

Lupus, trombosis e hidroxicloroquina M Law… M Petri, John Hopkins
Objetivos: Analizar factores de riesgo para primer episodio de
trombosis
Analizar papel de la HCQ y prednisona
“End point” primario: 1º episodio de trombosis arterial o
venosa
1795 pacientes (93% m, 56% caucásicas) SIN trombosis
10508 pacientes años:193 trombosis: 106 A, 83 V, 4 A y V
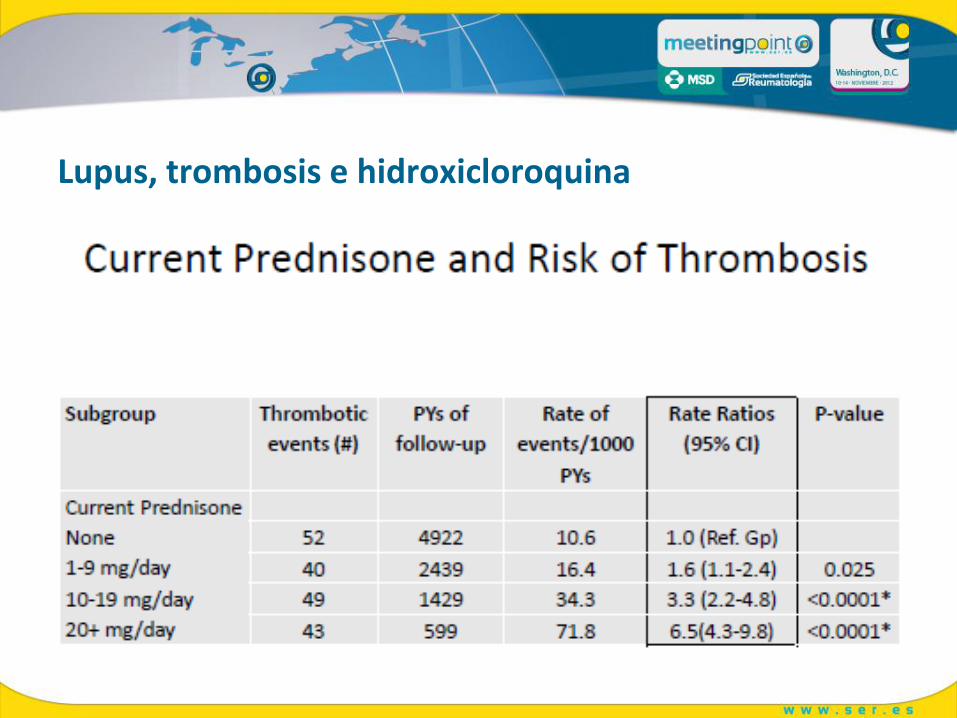
Lupus, trombosis e hidroxicloroquina
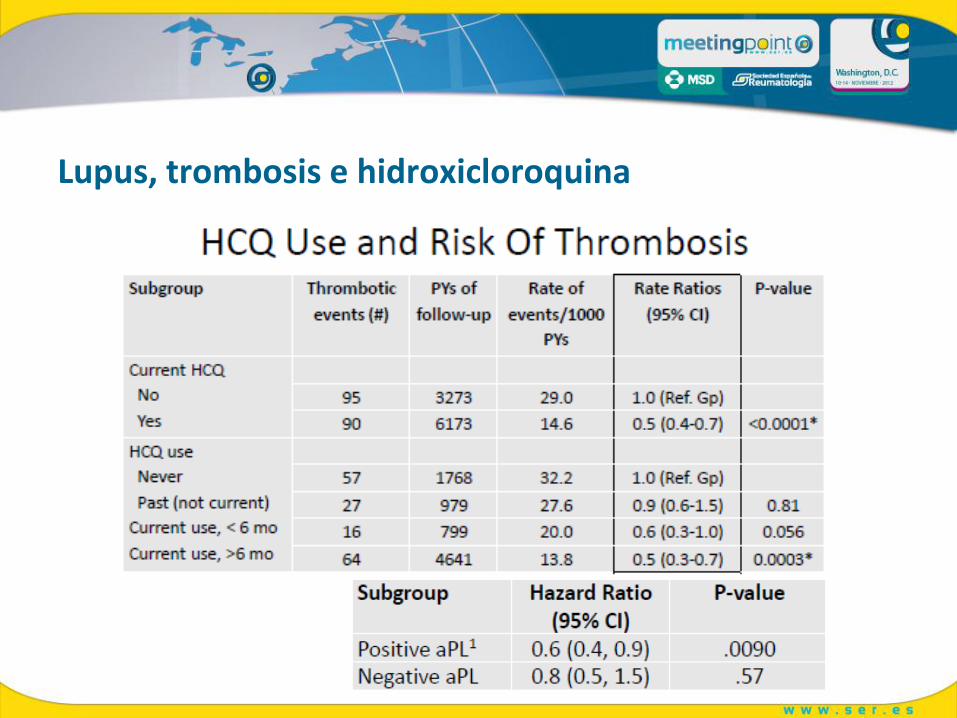
Lupus, trombosis e hidroxicloroquina
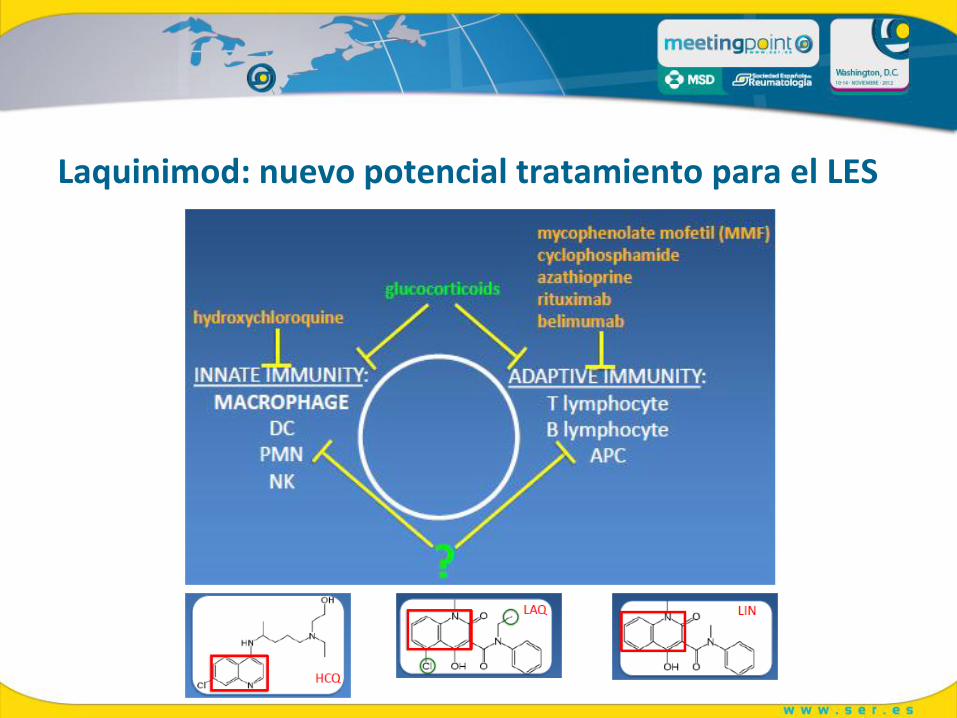
Laquinimod: nuevo potencial tratamiento para el LES
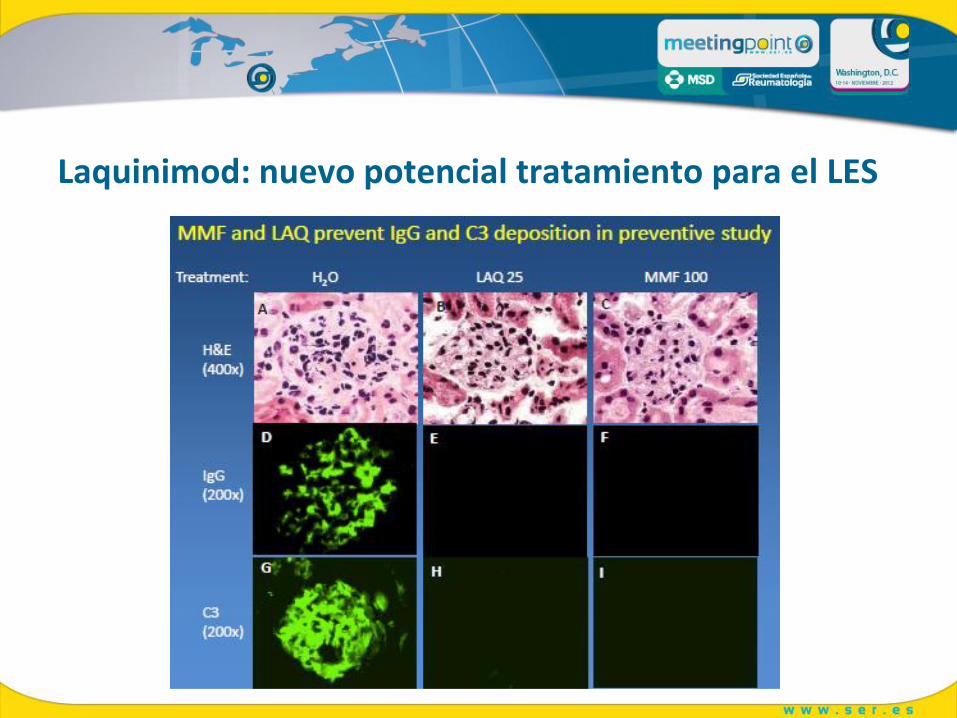
Laquinimod: nuevo potencial tratamiento para el LES
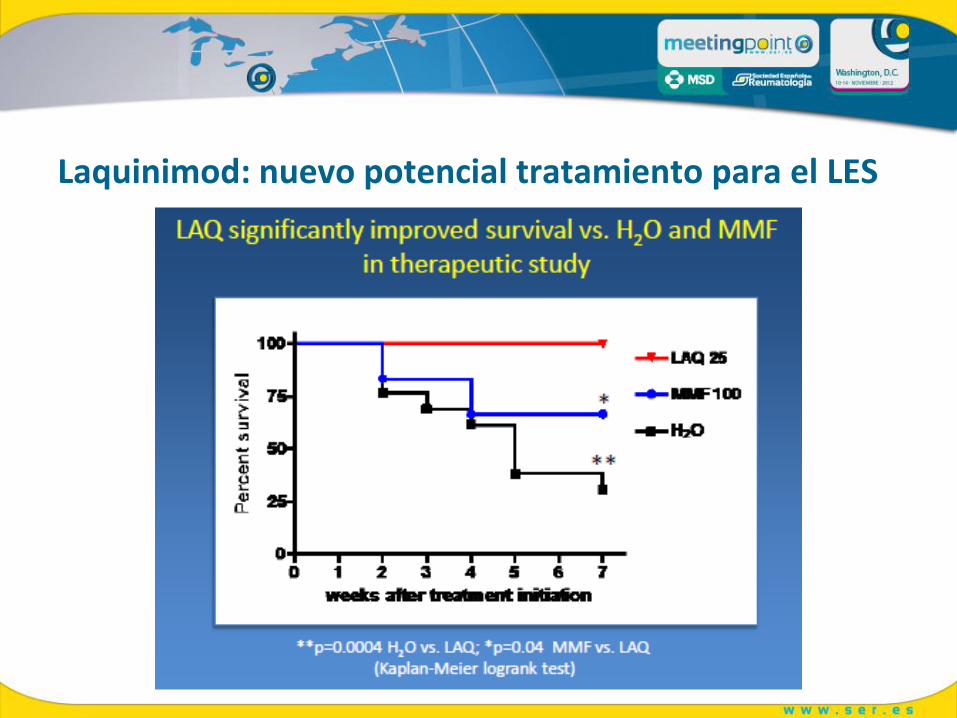
Laquinimod: nuevo potencial tratamiento para el LES
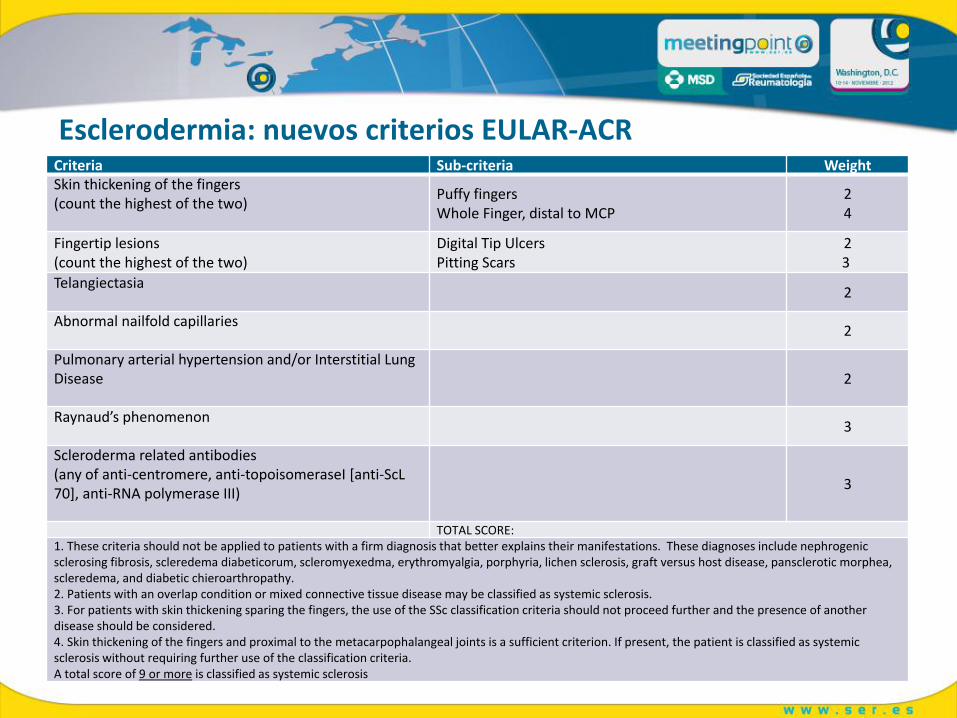
Esclerodermia: nuevos criterios EULAR-ACR Criteria Sub-criteria Weight Skin thickening of the fingers (count the highest of the two)
Puffy fingers Whole Finger, distal to MCP
2 4
Fingertip lesions (count the highest of the two)
Digital Tip Ulcers Pitting Scars
2 3
Telangiectasia
2
Abnormal nailfold capillaries
2
Pulmonary arterial hypertension and/or Interstitial Lung Disease
2
Raynaud’s phenomenon
3
Scleroderma related antibodies (any of anti-centromere, anti-topoisomeraseI [anti-ScL 70], anti-RNA polymerase III)
3
TOTAL SCORE: 1. These criteria should not be applied to patients with a firm diagnosis that better explains their manifestations. These diagnoses include nephrogenic sclerosing fibrosis, scleredema diabeticorum, scleromyexedma, erythromyalgia, porphyria, lichen sclerosis, graft versus host disease, pansclerotic morphea, scleredema, and diabetic chieroarthropathy. 2. Patients with an overlap condition or mixed connective tissue disease may be classified as systemic sclerosis. 3. For patients with skin thickening sparing the fingers, the use of the SSc classification criteria should not proceed further and the presence of another disease should be considered. 4. Skin thickening of the fingers and proximal to the metacarpophalangeal joints is a sufficient criterion. If present, the patient is classified as systemic sclerosis without requiring further use of the classification criteria. A total score of 9 or more is classified as systemic sclerosis