
Actualització en pròtesi del membre inferior: estandardització de la
prescripció protèsica
Dr. Lluís GUIRAO CANOServei de Rehabilitació
Hospital de Mataró
INTRODUCCIÓ

• Amputació MMII provoca canvis físics associats a limitacions funcionals:
– Alteracions en les transferències– Alteracions de equilibri– Alteracions en la marxa
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009
Especialment en nivells alts d’amputació
INTRODUCCIÓ

• Conseqüències limitacions funcionals:
– Reducció velocitat marxa– Increment despesa energètica– Asimetria de la marxa– Disminució de equilibri
Especialment en nivells alts d’amputació
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009
INTRODUCCIÓ
INTRODUCCIÓ
OBJECTIUS DE LA REHABILITACIÓ
capaç de passejar amb seguretat i de manera independent en superfícies planes, escales, rampes i voreres, amb o sense dispositius
d’ajuda
Berry D. Perceived stability, function and satisfaction among transfemoral amputees using microprocessor knee. JPO 2009

INTRODUCCIÓ
OBJECTIUS DE LA REHABILITACIÓ
capaç de passejar amb seguretat i de manera independent en superfícies planes, escales, rampes i voreres, amb o sense dispositius
d’ajuda
Berry D. Perceived stability, function and satisfaction among transfemoral amputees using microprocessor knee. JPO 2009
millora en la salut en general a través de l’augment en el nivell d’activitat
secundaria

OBJECTIUS PER LA MARXA
Limitades• Pròtesis
– Simples en el seu funcionament
– Menys costoses en preu
Michael JW. Prosthetic knees. The National Limb Loss Information Center. 2001

OBJECTIUS PER LA MARXA
Limitades• Pròtesis
– Simples en el seu funcionament
– Menys costoses en preu
Exigents• A mes exigència
d’activitat / marxa• Pròtesis més complexes i
costoses. • Cost d'un dispositiu
protèsic no és necessàriament en relació amb la seva idoneïtat
Michael JW. Prosthetic knees. The National Limb Loss Information Center. 2001

INTRODUCCIÓ
Èxit de la deambulació del pacient amputat
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009

‐ Bona adaptació de l’encaix
INTRODUCCIÓ
Èxit de la deambulació del pacient amputat
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009

‐ Bona adaptació de l’encaix ‐ Tractament rehabilitador
INTRODUCCIÓ
Èxit de la deambulació del pacient amputat
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009

‐ Bona adaptació de l’encaix ‐ Tractament rehabilitador‐ Nivell d’amputació (a mes distal, mes funcional)
INTRODUCCIÓ
Èxit de la deambulació del pacient amputat
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009

‐ Bona adaptació de l’encaix ‐ Tractament rehabilitador‐ Nivell d’amputació (a mes distal, mes funcional)‐ Correcta prescripció, alineació i disseny dels components protèsics.
INTRODUCCIÓ
Èxit de la deambulació del pacient amputat
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009

• % d'èxit en protetització en pacient geriàtric:
64 %tibials
4,5 %Desartic. genoll
31 %femoral
Fletcher D. Rehabilitation of the geriatric vascular amputee patient. Arch Phys Med Rehabil 2001
36 %TOTAL
INTRODUCCIÓ

• Quins son els motius?:
Expectatives altes dels pacients
Comorbilitats orgànica / psicològica
Funcions de pròtesis
inadequades
Fletcher D. Rehabilitation of the geriatric vascular amputee patient. Arch Phys Med Rehabil 2001
INTRODUCCIÓ

Fletcher D. Rehabilitation of the geriatric vascular amputee patient. Arch Phys Med Rehabil 2001
75% de totes las amputacions de EEII son > 65 anys
90% amputacions en geriatria son de causa vascular
60‐90% amputacions tibials i 50‐70% de
femorals en amputats geriàtrics: èxit protetizació
36% total
47 % tibials
14,5 % femorals
INTRODUCCIÓ

Vanieck N. Postural responses to dinamic perturbacions in amputee fallers versus nonfallers: a comparative study with able‐bodied subjects. Arch Phys Med Rehabil 2009.
Amputats MMII > risc caigudes que no amputats
(52% refereixen caiguda en els 12 mesos post amputació)
CAIGUDES I AMPUTACIÓ
debilitat muscular
inestabilitat postural
CAIGUDES

PROTETITZACIÓ
• La protetització pot restaurar moltes de les capacitats funcionals perdudes amb l’amputació
Brian J. Arch Phys Med Rehabil 2007

PROTETITZACIÓ
• La protetització pot restaurar moltes de les capacitats funcionalsperdudes amb l’amputació
• La selecció apropiada dels components protètics es una dels factors mes determinats en el grau de funció que pot ser restaurat
Brian J. Arch Phys Med Rehabil 2007

Edat, pes, nivell amputacióEtiologia amputacióNivell funcional previMotivació personalObjectius funcionals
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009
PROTETITZACIÓ
Elecció de components
factors

Hofstad CJ, Prescription of prosthetic ankle-foot mechanisms after lower limb amputation (Review). The Cochrane collaboration 2009
• Prescripció de dispositius protèsics– Necessitats funcionals de pacient
• Actiu / no actiu
• Treballa
• A on viu
• Comorbilitats, traumàtic / vascular
PROTETITZACIÓ

Hofstad CJ, Prescription of prosthetic ankle-foot mechanisms after lower limb amputation (Review). The Cochrane collaboration 2009
• Prescripció de dispositius protèsics– Necessitats funcionals de pacient
• Actiu / no actiu
• Treballa
• A on viu
• Comorbilitats, traumàtic / vascular
– Aspectes tècnics i funcionals dels dispositius• Complexitat
• Disponibilitat de tècnic ortopeda
PROTETITZACIÓ
INDICACIÓ PRESCRIPCIÓ PROTÈSICA
INDIVIDUAL
CORRECTA ELECCIÓ COMPONENTS PROTÈSICS
INFLUENCIAR EL NIVELL FUNCIONAL K FINAL
PROTETITZACIÓ

• Dispositius protèsics
• Velocitat marxa• Reducció VO2• Augmenten perímetre de la marxa• Augmenta simetria de la petxada• Augmenta velocitat • Millora equilibri dinàmic i estàtic
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009
PROTETITZACIÓ

INDEPENDENCIA PER LES AVD
Moderat suport familiarnecessita caminar un mínim de 600 passos/dia per viure en pis o apartament i realitzar les AVD.
Lerner‐Frankiel MB. Functional community ambulation: what are your criteria? Clin Management 1986.

INDEPENDENCIA PER LES AVD
Moderat suport familiarnecessita caminar un mínim de 600 passos/dia per viure en pis o apartament i realitzar les AVD.
• Per viure independentment sense suport extern i realitzant algunes activitats fora de casa, hauria de caminar entre 1100 y 1450 passos/dia.
Lerner‐Frankiel MB. Functional community ambulation: what are your criteria? Clin management 1986.

DESPESA ENERGÈTICA
Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
Pacients amputats caminen mes lents i amb mes VO2que els NO amputats
VO2 augmenta en relació al nivell d’amputació
Funcionalitat diferent
– Despesa energètica
• 40% mes en amputat transfemoral
• 20% mes en amputat transtibial
• 5 – 10% amputat a nivell Syme
Pitetti K. Amputation and exercise. National Center on physical activity, 2007
DESPESA ENERGÈTICA
Funcionalitat diferent
– Despesa energètica
• 40% mes en amputat transfemoral
• 20% mes en amputat transtibial
• 5 – 10% amputat a nivell Syme
Pitetti K. Amputation and exercise. National Center on physical activity, 2007
DESPESA ENERGÈTICA
L’augment del cost energètic en marxa, major esforç per caminar, disminució del temps en caminar
contribueix a estil de vida sedentari
Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
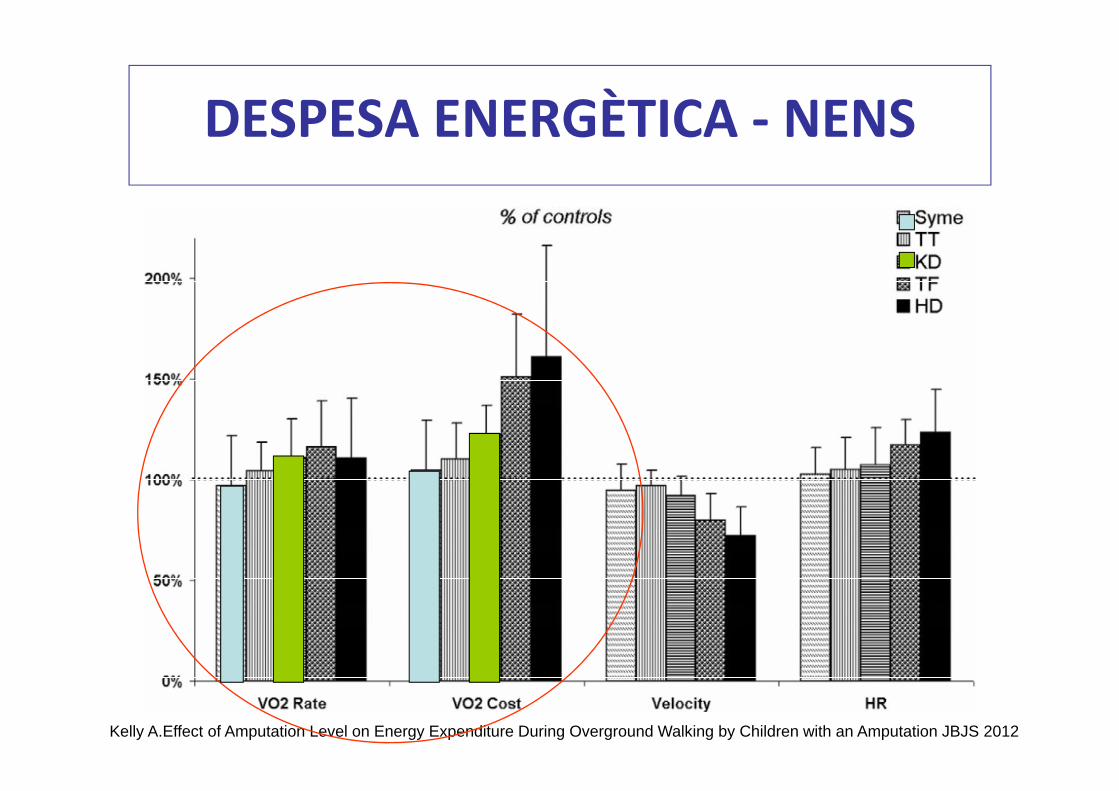
DESPESA ENERGÈTICA ‐ NENS

Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
DESPESA ENERGÈTICA ‐ NENS

Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
DESPESA ENERGÈTICA ‐ NENS

Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
DESPESA ENERGÈTICA ‐ NENS

Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
DESPESA ENERGÈTICA ‐ NENS

Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
DESPESA ENERGÈTICA ‐ NENS

Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
DESPESA ENERGÈTICA ‐ NENS
• Syme, tibials i desarticulats de genoll– caminen a la mateixa velocitat que els NO amputats
– SENSE incrementar el seu VO2.
CONCLUSIONS

Kelly A.Effect of Amputation Level on Energy Expenditure During Overground Walking by Children with an Amputation JBJS 2012
DESPESA ENERGÈTICA ‐ NENS
• Syme, tibials i desarticulats de genoll– caminen a la mateixa velocitat que els NO amputats
– SENSE incrementar el seu VO2.
• Femorals i desarticulats de maluc– caminen mes lentament
– AMB increment de VO2
CONCLUSIONS

Waters R. The Energy Expenditure of Amputee Gait. Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles 2002
DESPESA ENERGÈTICA ‐ ADULTS
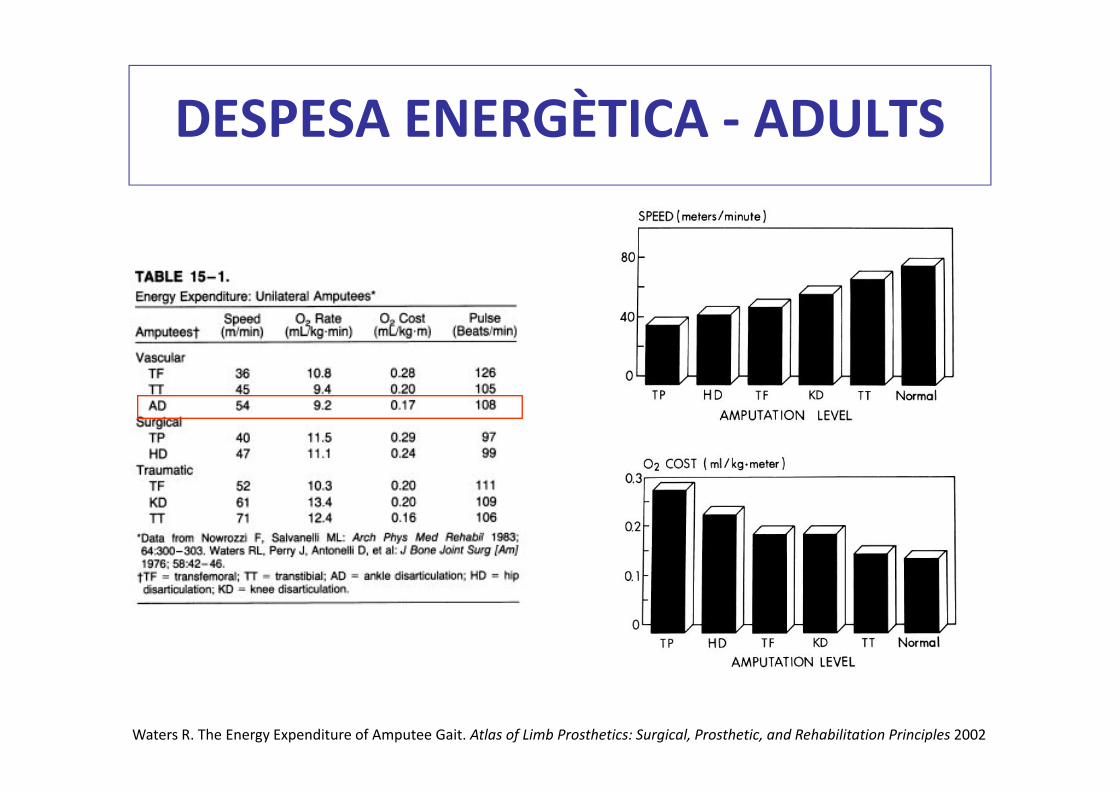
Waters R. The Energy Expenditure of Amputee Gait. Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles 2002
DESPESA ENERGÈTICA ‐ ADULTS

Waters R. The Energy Expenditure of Amputee Gait. Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles 2002
DESPESA ENERGÈTICA ‐ ADULTS
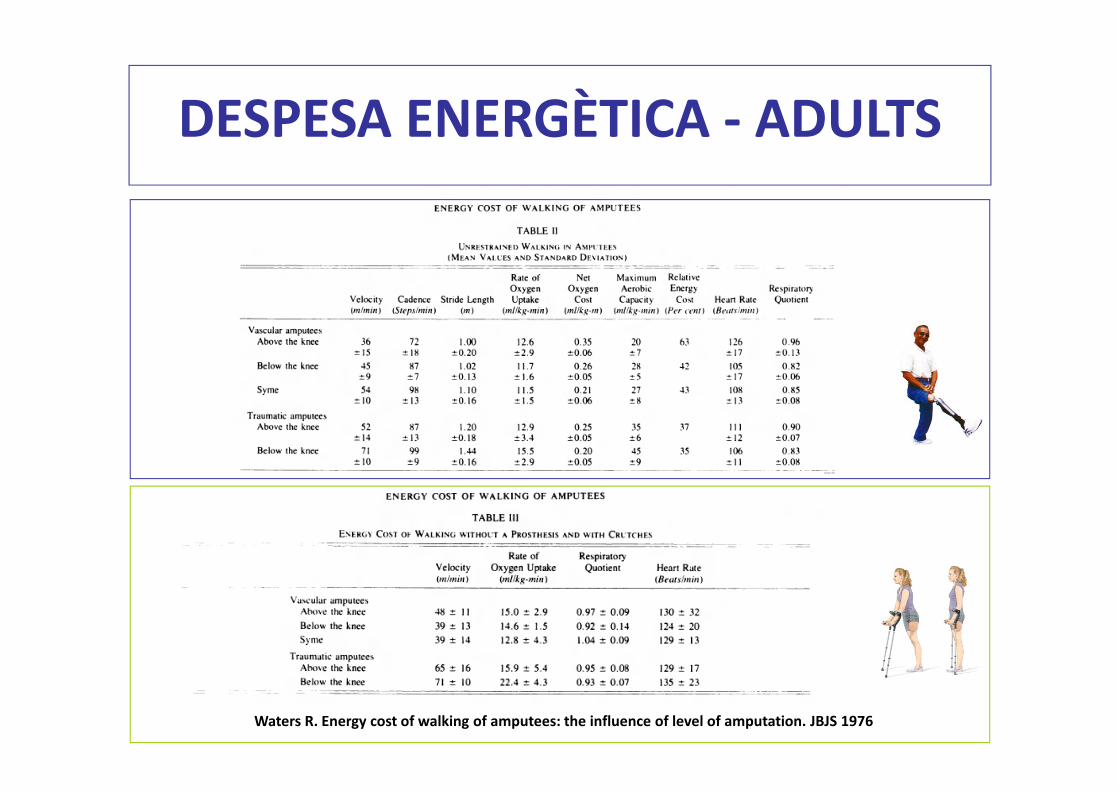
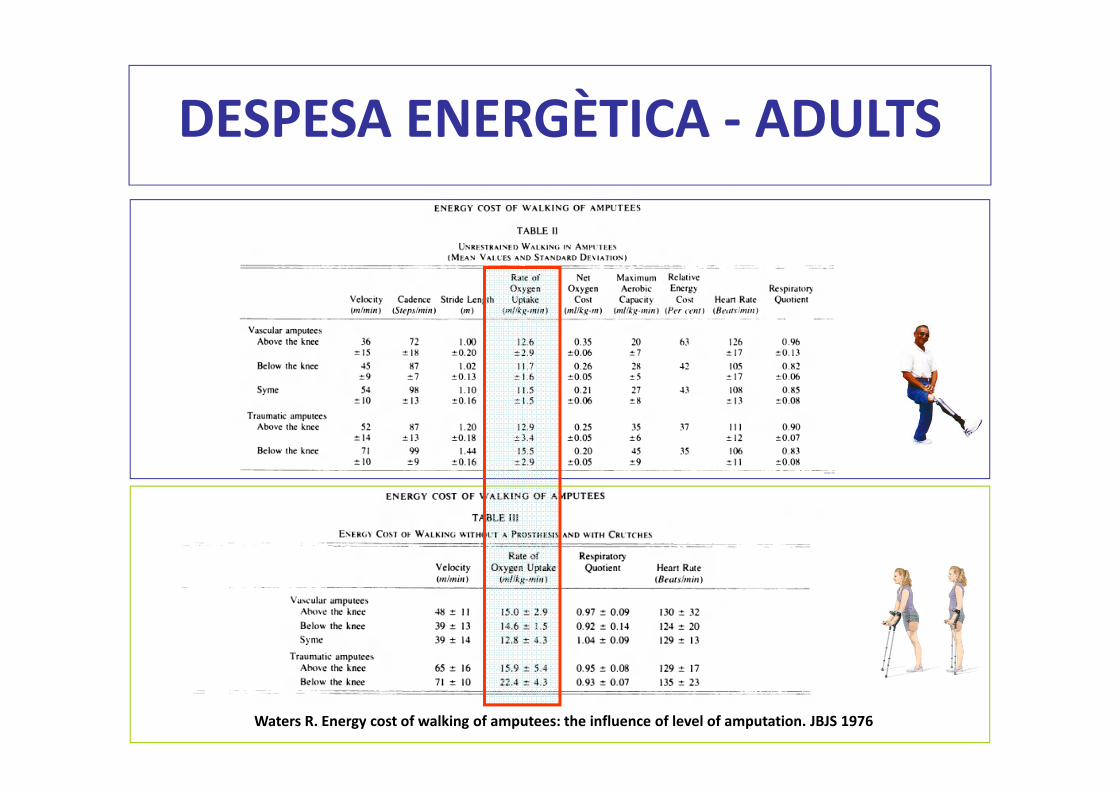
Waters R. Energy cost of walking of amputees: the influence of level of amputation. JBJS 1976
DESPESA ENERGÈTICA ‐ ADULTS
Waters R. Energy cost of walking of amputees: the influence of level of amputation. JBJS 1976
DESPESA ENERGÈTICA ‐ ADULTS

DESPESA ENERGÈTICA ‐ ADULTS
• ORIGEN VASCULAR– Syme / Tibial
• Tasa VO2: 42%
• Capacitat aeròbica máxima: 43%
– Subjectes controls• Majors 60 anys
• 41%
• ORIGEN TRAUMÀTIC– Tibial
• Tasa VO2: 35%
– Femoral• Tasa VO2: 37%
– Subjectes controls• Majors 30 anys • 34%
Waters R. Energy cost of walking of amputees: the influence of level of amputation. JBJS 1976
CONCLUSIONS

DESPESA ENERGÈTICA ‐ ADULTS
Waters R. Energy cost of walking of amputees: the influence of level of amputation. JBJS 1976
VASCULAR TRAUMÀTIC
Modificació de la velocitat de la marxa per mantenir el VO2 dins de valors normals, excepte
femorals vasculars

Goktepe A. Energy expenditure of walking with prostheses: comparison of three amputation levels. Prosthetic and Orthot 2010
DESPESA ENERGÈTICA ‐ PEU

Goktepe A. Energy expenditure of walking with prostheses: comparison of three amputation levels. Prosthetic and Orthot 2010
DESPESA ENERGÈTICA ‐ PEU

• Importància de la càrrega distal:
– Desarticulació genoll
– Desarticulació de turmell (Syme)
– Millores quirúrgiques:
•Ertl Amputation
•Grittie Stokes
•Implant Femoral (Assaig Clínic Hospital de Mataró)
RECOLZAMENT DISTAL


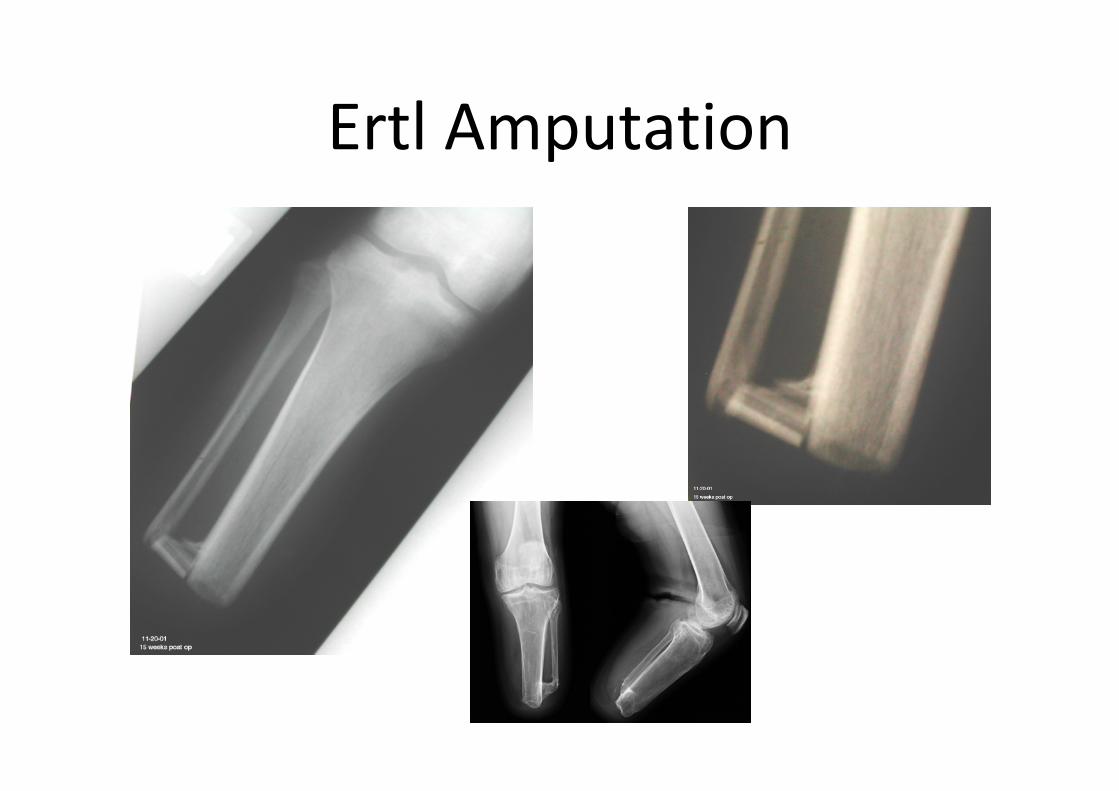
Ertl Amputation

Grittie Stokes
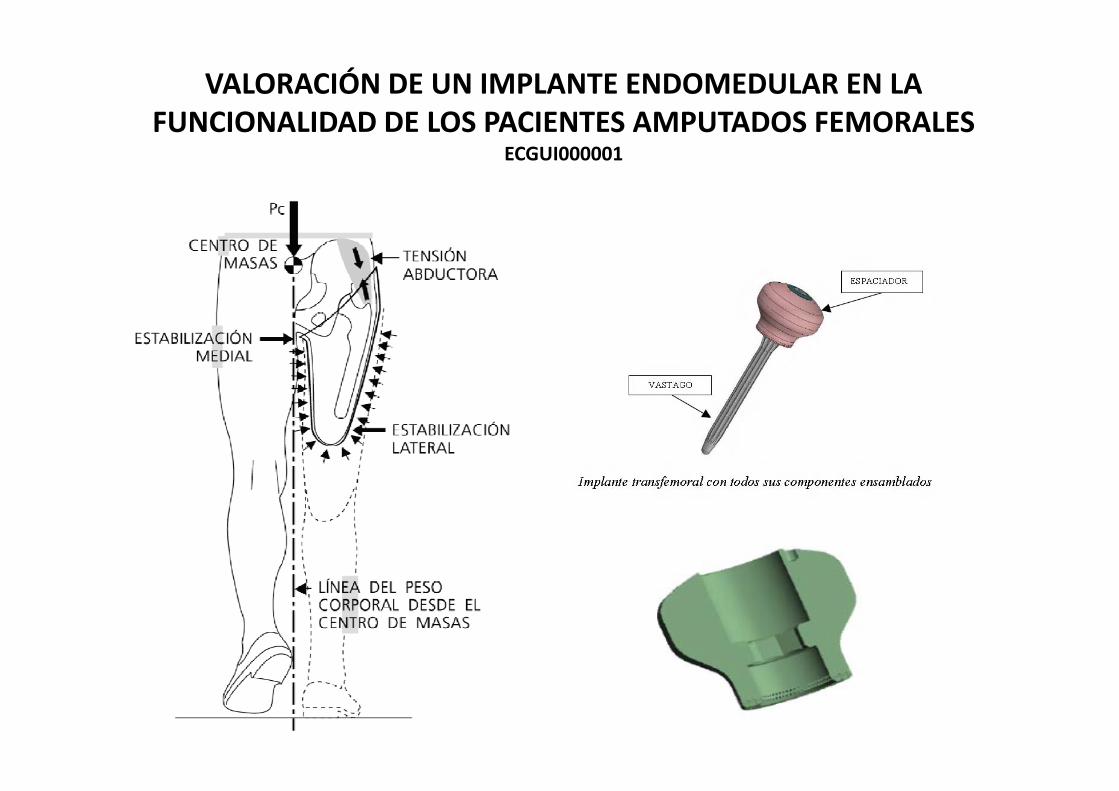
VALORACIÓN DE UN IMPLANTE ENDOMEDULAR EN LA FUNCIONALIDAD DE LOS PACIENTES AMPUTADOS FEMORALES
ECGUI000001




Millora‐Metres i velocitat de la marxa‐DMO del coll femoral‐VO2‐Satisfacció ‐Qualitat de vida

INDICACIONS EN LA PRESCRIPCIÓ

INDICACIONS EN LA PRESCRIPCIÓ

INDICACIONS EN LA PRESCRIPCIÓ

INDICACIONS EN LA PRESCRIPCIÓ

INDICACIONS EN LA PRESCRIPCIÓ
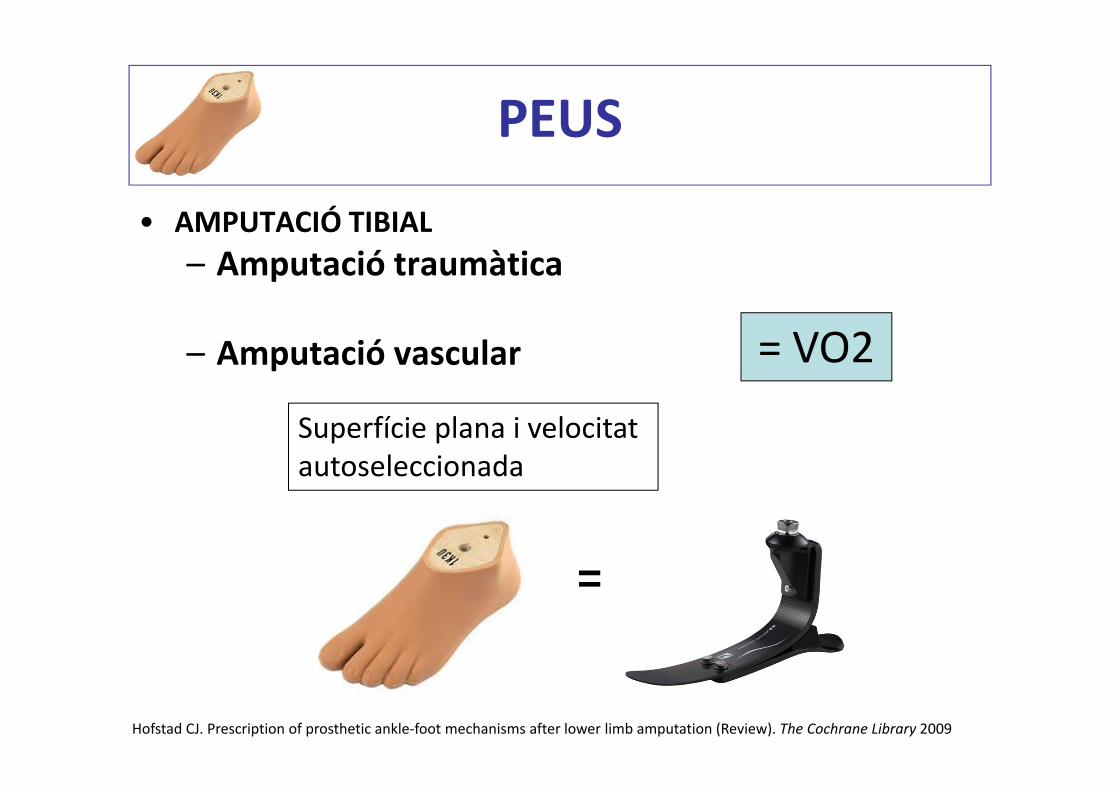
• AMPUTACIÓ TIBIAL– Amputació traumàtica
– Amputació vascular
Hofstad CJ. Prescription of prosthetic ankle‐foot mechanisms after lower limb amputation (Review). The Cochrane Library 2009
PEUS
=
= VO2
Superfície plana i velocitat autoseleccionada

• AMPUTACIÓ TIBIAL– Amputació traumàticacaminava > peu Flex vs peu SACH
– Amputació vascularmajor velocitat elegida al caminar amb peu Flex vs peu SACH
– 77,8±16,9m/min vs 71,4±15,8m/min
– 71,6±12,6m/min vs 63,6±10,0m/min
Hofstad CJ. Prescription of prosthetic ankle‐foot mechanisms after lower limb amputation (Review). The Cochrane Library 2009
PEUS
• Amputació transfemoral
• Activitat intensa
– Peu fibra carbó ‐ Peu SACH
Hofstad CJ. Prescription of prosthetic ankle‐foot mechanisms after lower limb amputation (Review). The Cochrane Library 2009
‐Menor VO2
‐Major eficiència de la marxa
PEUS
• Conclusions– A velocitat lenta no hi ha diferencies entre peu SACH i Fibra carbó (VO2).
– A major velocitat o pendents / rampes, les diferències son significatives.
Hofstad CJ. Prescription of prosthetic ankle‐foot mechanisms after lower limb amputation (Review). The Cochrane Library 2009
PEUS

• Conclusions– A velocitat lenta no hi ha diferencies entre peu SACH i Fibra carbó (VO2).
– A major velocitat o pendents / rampes, les diferències son significatives.
Prescripció de peus fibra carbó
Hofstad CJ. Prescription of prosthetic ankle‐foot mechanisms after lower limb amputation (Review). The Cochrane Library 2009
PEUS
Pacients actius que poden alterar velocitat i fer desnivells / rampes / pendents
Tant en pacient femoral com
tibial
Tant en grup vascular com
traumàtic

Brian J. Arch Phys Med Rehabil 2007
GENOLLS
Funcions:
‐Estabilitzar
‐Controlar eficaçment la marxa

Isakov E. Energy expenditure and cardiac response in above knee amputees while using prostheses with open and locked knee mecanisms. Scand J Rehabil Med 1985
• 17 pacients femoral: 14 > 50 anys
• Walking test• Mesura: FC, velocitat marxa i
Consum O2
• Resultats:– Disminució FC amb GB– Velocitat confortable marxa > en GB q GL en > 50 anys; contrari en joves
– Consum oxigen > GL
GENOLLS
Son utilitat els genolls de bloqueig?

• Conclusions:– Genoll bloqueig recomanada per pacients grans que no pot caminar a velocitats altes i amb menor esforç.
– Genoll lliure recomanada per pacients joves per la seva millor condició física que fa que caminin a velocitats mes altes (encara que consum O2 i FC sigui mes alta).
GENOLLS
Isakov E. Energy expenditure and cardiac response in above knee amputees while using prostheses with open and locked knee mecanisms. Scand J Rehabil Med 1985

Devlin M. Patient preference and gait efficiency in a geriatric popularion with transfemoral amputation. Arch Phys Med Rehabil 2002
GENOLLS
no diferencies en VO2 ni velocitat
marxa
pròtesi amb genollbloqueig en amputat geriàtricmarxa mes
eficient (VO2) vs genoll lliure
Son utilitat els genolls de bloqueig?

• 9 pacients amputats femorals grans
• Walking test• No diferències en requeriments energètics per la deambulació amb genoll bloqueig o lliure
Traugh GH. Energy expenditure of ambulation in patients with above knee amputations. Arch Phys Med Rehabil 1975
GENOLLS
Son utilitat els genolls de bloqueig?

• Millores en:– Simetria de la marxa– Carrega del cantó protèsic– Reducció càrrega del cantó
contralateral: “sana”– Millor seguretat al pujar /
baixar escales
Son utilitat els genolls amb microprocesador?
Bellman M. Comparative biomechanical analysis of current microprocessor controlled prosthetic knee joints. Arch Phys Med Rehabil 2010
GENOLLS
Disminueix el nombre de caigudes
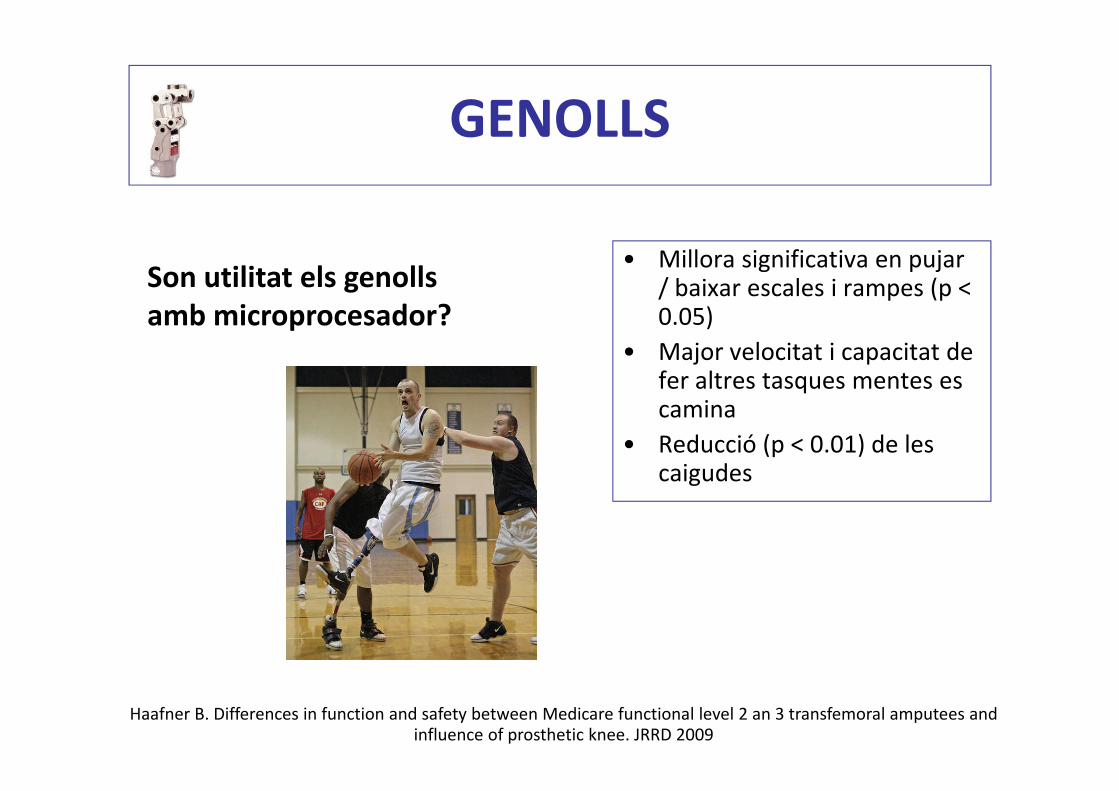
• Millora significativa en pujar / baixar escales i rampes (p < 0.05)
• Major velocitat i capacitat de fer altres tasques mentes es camina
• Reducció (p < 0.01) de les caigudes
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009
GENOLLS
Son utilitat els genolls amb microprocesador?

• Millora significativa en pujar / baixar escales I rampes (p < 0.05)
• Major velocitat I capacitat de fer altres tasques mentes es camina
• Reducció (p < 0.01) de les caigudes
Haafner B. Differences in function and safety between Medicare functional level 2 an 3 transfemoral amputees and influence of prosthetic knee. JRRD 2009
GENOLLS
Son utilitat els genolls amb microprocesador?
50% de K2
33% de K3 Nivel K

• Millors resultats funcionals
• Increment de l’activitat física per exteriors
• Millora en qualitat de vida
Kenton R Energy Expenditure and Activity of Transfemoral Amputees Using Mechanical and Microprocessor‐Controlled Prosthetic Knees Arch Phys Med Rehabil 2008
GENOLLS
Microprocesador vs genolls hidràulics?
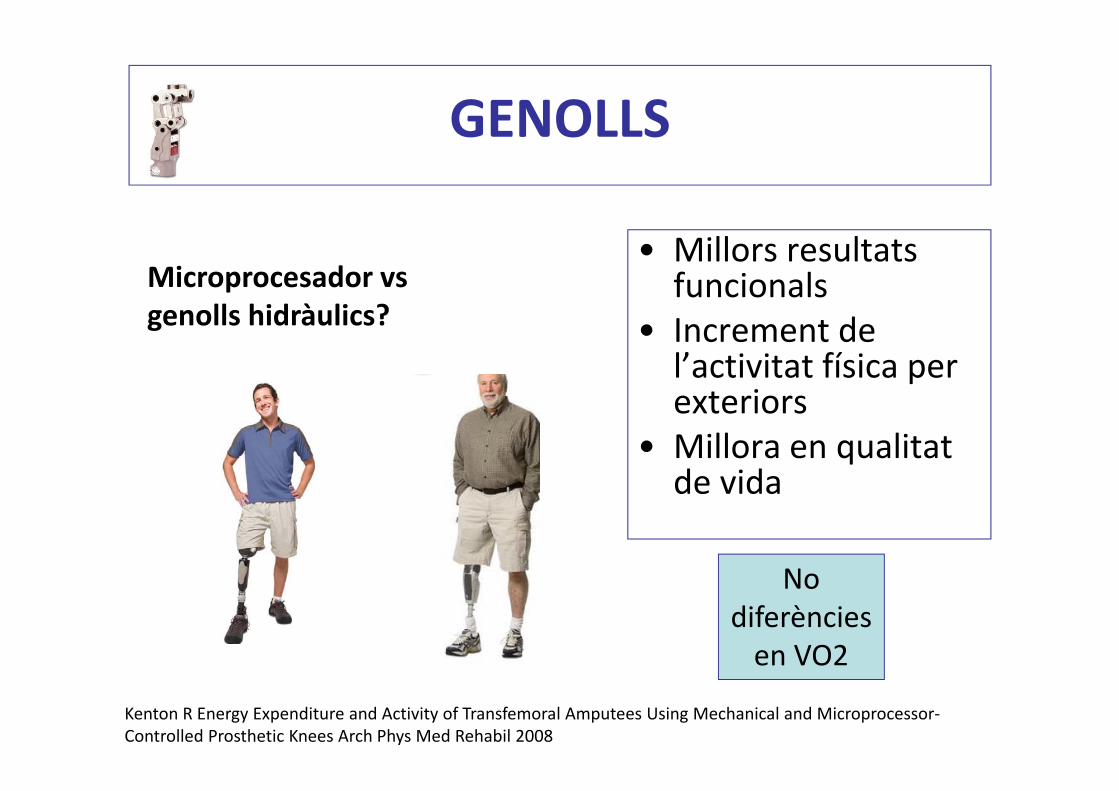
• Millors resultats funcionals
• Increment de l’activitat física per exteriors
• Millora en qualitat de vida
Kenton R Energy Expenditure and Activity of Transfemoral Amputees Using Mechanical and Microprocessor‐Controlled Prosthetic Knees Arch Phys Med Rehabil 2008
GENOLLS
Microprocesador vs genolls hidràulics?
No diferències en VO2

• 40% des pacients amputats pateixen problemes cutanis
• Us prolongat de l’encaix es el principal causant de las úlceres
• Els pacients mes actius tenen mes riscos de desenvolupar problemes en la pell (45‐63%)
Dudek N, Meridith M, Shawn C. Dermatologic conditions associated with use of a lower‐extremity prothesis. Arh Phys Med Rehabil 2005
ENCAIXOS

ENCAIXOS

Causes mes freqüents de percepció negativa de salut i mobilitat en el pacient (33 – 45%)
• Tant en sedestació com en bipedestació
Hagbert K, Branemark R, Gunterberg B, Rydevik B. Osseointegrated trans‐femoralamputation prostheses: prospective results of general and condition‐specific quality of live in 18 patients at 2 year follow‐up. Prosthetics and Orthotics International 2008
ENCAIXOS
Disconfort secundari a l’encaix
Encaix mes utilitzat: quadrangular
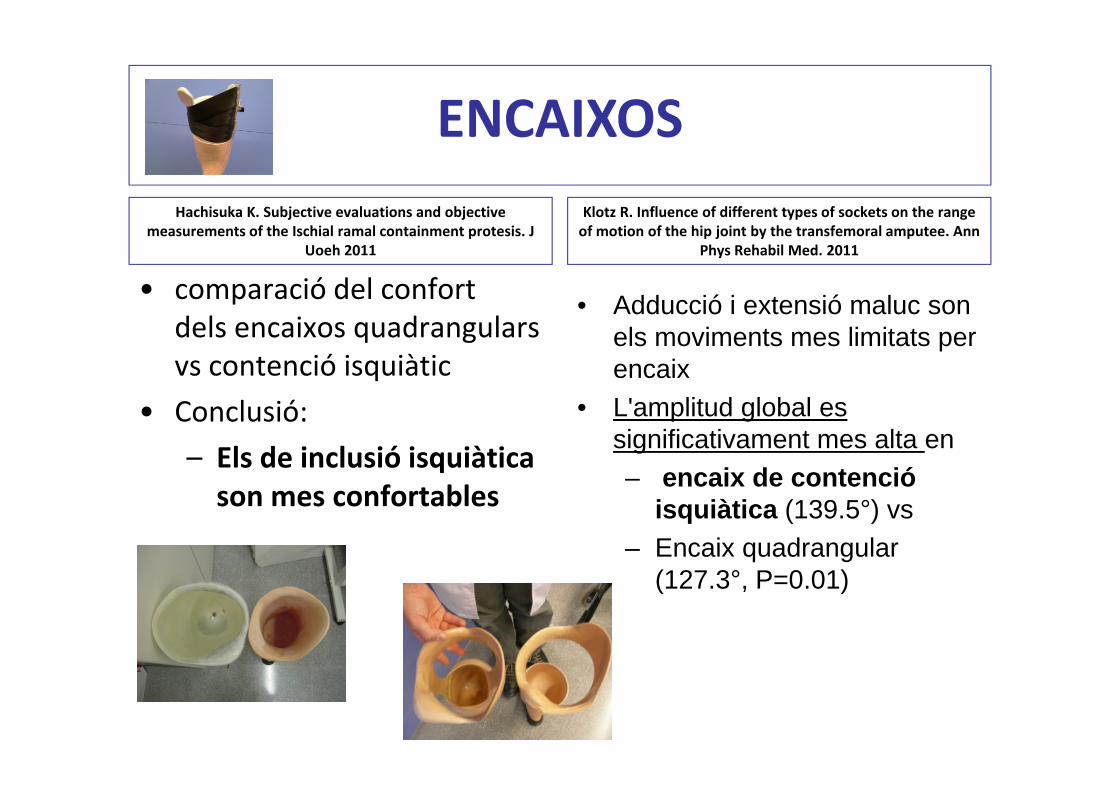
Hachisuka K. Subjective evaluations and objective measurements of the Ischial ramal containment protesis. J
Uoeh 2011
• comparació del confort dels encaixos quadrangulars vs contenció isquiàtic
• Conclusió:
– Els de inclusió isquiàtica son mes confortables
ENCAIXOS
Hachisuka K. Subjective evaluations and objective measurements of the Ischial ramal containment protesis. J
Uoeh 2011
• comparació del confort dels encaixos quadrangulars vs contenció isquiàtic
• Conclusió:
– Els de inclusió isquiàtica son mes confortables
Klotz R. Influence of different types of sockets on the range of motion of the hip joint by the transfemoral amputee. Ann
Phys Rehabil Med. 2011
• Adducció i extensió maluc son els moviments mes limitats per encaix
• L'amplitud global es significativament mes alta en– encaix de contenció
isquiàtica (139.5°) vs– Encaix quadrangular
(127.3°, P=0.01)
ENCAIXOS

Gailey RS. The CAT‐CAM socket and quadrilateral socket: a comparison of energy cost during ambulation. Prosthet Orthot Int. 1993
ENCAIXOS
• Diferències significatives en VO2 i FC en velocitat lentes(48m/min) i altes(97m/min) amb encaix CAT CAM (p< 0.01)
Major VO2 en encaix quadrangular a velocitat
altes vs CAT CAM

Hospital de Mataró Femoral Socket


Sadeeq Ali, Qualitative Study of Prosthetic Suspension Systems on Transtibial Amputees’ Satisfaction and Perceived Problems With Their Prosthetic Devices Arch Phys Med Rehabl 2012
SILICONES
• Comparació 3 tipus de sistemes de suspensió– Polietilè
– Silicona amb pin
– Silicona amb Seal‐In
• Satisfacció i percepció de problemes (n=243)
• Pacients tibials

Sadeeq Ali, Qualitative Study of Prosthetic Suspension Systems on Transtibial Amputees’ Satisfaction and Perceived Problems With Their Prosthetic Devices Arch Phys Med Rehabl 2012
SILICONES
• Silicona pin / Seal In > Polietilè
• Silicona pin > suor
• El millor puntuat i menys problemes va ser SEAL – IN– Excep en la col∙locació de la silicona

• Resultats de 2MWT no van ser influenciats per l’augment de pes:– 53.4+/‐28.4m ‐‐‐ 150g
– 55.1+/‐28.9m ‐‐‐ 770g
– 52.8+/‐26.7m ‐‐‐1625g
• > 50% dels pacients van preferir la pròtesi de 770g que la de 150g
Meikle B Does increased prosthetic weight affect gait speed and patient preference in dysvascular transfemoral amputees? Arch Phys Med Rehabil 2003
PES DE LA PRÒTESI

• Protetització “standard”
• No individualitzem
• La edat no es una factor limitant
• Beneficis del recolzament distal–Nivell amputació o quirúrgics
–V02, FC, velocitat marxa
CONCLUSIONS
• Dispositius: canvis de nivell K
• Peus fibra carbó disminueixen VO2 en pacients amb canvis velocitat
• Genolls de bloqueig: – indicació en pacients nivell K1/2
• Genoll microprocessador
CONCLUSIONS
• Encaix quadrangular mes freqüent
• Encaix CAT CAM es –mes confortable
– limita menys BA maluc
–menys VO2
• Se‐In te menys problemes
CONCLUSIONS

MOLTES GRÀCIES!!







